Get your patient on Tromethamine - Tromethamine injection, Solution (Tromethamine)
Tromethamine - Tromethamine injection, Solution prescribing information
INDICATIONS AND USAGE
Tromethamine Injection is indicated for the prevention and correction of metabolic acidosis. In the following conditions it may help to sustain vital functions and thus provide time for treatment of the primary disease:
- Metabolic Acidosis Associated with Cardiac Bypass Surgery.
- Tromethamine Injection has been found to be primarily beneficial in correcting metabolic acidosis which may occur during or immediately following cardiac bypass surgical procedures.
- Correction of Acidity of ACD Blood in Cardiac Bypass Surgery.
- It is well known that ACD blood is acidic and becomes more acidic on storage. Tromethamine effectively corrects this acidity. Tromethamine Injection may be added directly to the blood used to prime the pump-oxygenator. When ACD blood is brought to a normal pH range the patient is spared an initial acid load. Additional tromethamine may be indicated during cardiac bypass surgery should metabolic acidosis appear.
- Metabolic Acidosis Associated with Cardiac Arrest.
- Acidosis is nearly always one of the consequences of cardiac arrest and, in some instances, may even be a causative factor in arrest. It is important therefore, that the correction of acidosis should be started promptly with other resuscitative efforts. By correcting acidosis, Tromethamine injection has caused the arrested heart to respond to resuscitative efforts after standard methods alone had failed. In these cases, tromethamine was given intraventricularly. It is to be noted, however, that such precariously ill patients often have died subsequently of causes unrelated to the administration of tromethamine. With administration by the peripheral venous route, metabolic acidosis has been corrected in a majority of patients. The success in reinstitution of cardiac rhythm by this means probably has not been of the same order of magnitude as with the intraventricular route.
DOSAGE AND ADMINISTRATION
Tromethamine Injection is administered by slow intravenous infusion, by addition to pump-oxygenator ACD blood or other priming fluid or by injection into the ventricular cavity during cardiac arrest. For infusion by peripheral vein, a large needle should be used in the largest antecubital vein or an indwelling catheter placed in a large vein of an elevated limb to minimize chemical irritation of the alkaline solution during infusion. Catheters are recommended.
Dosage and rate of administration should be carefully supervised to avoid overtreatment (alkalosis). Pretreatment and subsequent determinations of blood values (e.g. pH, PCO 2 , PO 2 , glucose and electrolytes) and urinary output should be made as necessary to monitor dosage and progress of treatment. In general, dosage should be limited to an amount sufficient to increase blood pH to normal limits (7.35 to 7.45) and to correct acid-base derangements. The total quantity to be administered during the period of illness will depend upon the severity and progression of the acidosis. The possibility of some retention of tromethamine, especially in patients with impaired renal function, should be kept in mind.
The intravenous dosage of Tromethamine Injection may be estimated from the buffer base deficit of the extracellular fluid in mEq/liter determined by means of the Siggaard-Andersen nomogram. The following formula is intended as a general guide:
Tromethamine Injection (mL of 0.3 M) Required =
Body Weight (kg) X
Base Deficit (mEq/liter) X 1.1•
Thus, a 70 kg patient with a buffer base deficit (“negative base excess”) of 5 mEq/liter would require 70 x 5 x 1.1 = 385 mL of Tromethamine Injection containing 13.9 g (115 mEq) of tromethamine. The need for administration of additional Tromethamine Injection is determined by serial determinations of the existing base deficit.
• Factor of 1.1 accounts for an approximate reduction of 10% in buffering capacity due to the presence of sufficient acetic acid to lower pH of the 0.3 M solution to approximately 8.6.
Correction of Metabolic Acidosis Associated with Cardiac Bypass Surgery: An adverse dose of approximately 9.0 mL/kg (324 mg/kg) has been used in clinical studies with Tromethamine Injection. This is equivalent to a total dose of 630 mL (189 mEq) for 70 kg patient. A total single dose of 500 mL (150 mEq) is considered adequate for most adults. Larger single doses (up to 1000 mL) may be required in unusually severe cases.
It is recommended that individual doses should not exceed 500 mg/kg (227 mg/lb) over a period of not less than one hour. Thus, for a 70 kg (154 pound) patient the dose should not exceed a maximum of 35 g per hour (1078 mL of a 0.3 M solution). Repeated determinations of pH and other clinical observations should be used as a guide to the need for repeat doses.
Correction of Acidity of ACD Blood in Cardiac Bypass Surgery: The pH of stored blood ranges from 6.80 to 6.22 depending upon the duration of storage. The amount of Tromethamine Injection used to correct this acidity ranges from 0.5 to 2.5 g (15 to 77 mL of a 0.3 M solution) added to each 500 mL of ACD blood used for priming the pump-oxygenator. Clinical experience indicates that 2 g (62 mL of a 0.3 M solution) added to 500 mL of ACD blood is usually adequate.
Correction of Metabolic Acidosis Associated with Cardiac Arrest: In the treatment of cardiac arrest, Tromethamine Injection should be given at the same time that other standard resuscitative measures, including manual systole, are being applied. If the chest is open, Tromethamine Injection is injected directly into the ventricular cavity. From 2 to 6 g (62 to 185 mL of a 0.3 M solution) should be injected immediately. Do not inject into the cardiac muscle .
If the chest is not open, from 3.6 to 10.8 g (111 to 333 mL of a 0.3 M solution) should be injected immediately into a larger peripheral vein. Additional amounts may be required to control acidosis persisting after cardiac arrest is reversed.
Correction of Metabolic Acidosis Associated with RDS in Neonates and Infants: The initial dose of Tromethamine Injection should be based on initial pH and birthweight amounting to approximately 1 mL per kg for each pH unit below 7.4. Further doses have been given according to changes in PaO 2 , pH and PCO 2 .
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. (See CONTRAINDICATIONS ).
CONTRAINDICATIONS
Tromethamine Injection is contraindicated in uremia and anuria. In neonates it is also contraindicated in chronic respiratory acidosis and salicylate intoxication.
ADVERSE REACTIONS
Generally, side effects have been infrequent.
Respiratory: Although the incidence of ventilatory depression is low, it is important to keep in mind that such depression may occur. Respiratory depression may be more likely to occur in patients who have chronic hypoventilation or those who have been treated with drugs which depress respiration. In patients with associated respiratory acidosis, tromethamine should be administered with mechanical assistance to ventilation.
Vascular: Extreme care should be taken to avoid perivascular infiltration. Local tissue damage and subsequent sloughing may occur if extravasation occurs. Chemical phlebitis and venospasm also have been reported.
Hematologic: Transient depression of blood glucose may occur.
Hepatic: Infusion via low-lying umbilical venous catheters has been associated with hepatocellular necrosis.
Reactions which may occur because of the solution or the technique of administration include febrile response, infection at the site of injection, venous thrombosis or phlebitis extending from the site of injection extravasation and hypervolemia.
If an adverse reaction does occur, discontinue the infusion, evaluate the patient, institute appropriate therapeutic countermeasures and save the remainder of the fluid for examination if deemed necessary.
DESCRIPTION
Tromethamine Injection is a sterile, nonpyrogenic 0.3 M solution of tromethamine, adjusted to a pH of approximately 8.6 with glacial acetic acid. It is administered by intravenous injection, by addition to ACD blood for priming cardiac bypass equipment and by injection into the ventricular cavity during cardiac arrest.
Each 100 mL contains tromethamine 3.6 g (30 mEq) in water for injection. The solution is hypertonic 389 mOsmol/L (calc.). pH 8.6 (8.4-8.8).
Tromethamine Injection contains no bacteriostat, antimicrobial agent or added buffer (except acetic acid for pH adjustment) and is intended only for use as a single-dose injection. When smaller doses are required the unused portion should be discarded.
Tromethamine Injection is a parenteral systemic alkalizer and fluid replenisher.
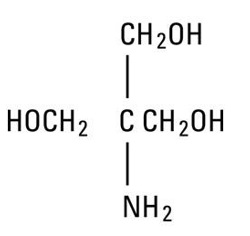
Tromethamine, USP (sometimes called “tris” or “tris buffer”) is chemically designated 2-amino-2- (hydroxymethyl)-1, 3-propanediol, a solid readily soluble in water, also classified as an organic amine buffer. It has the following structural formula:
Water for Injection, USP is chemically designated H 2 O.
CLINICAL PHARMACOLOGY
When administered intravenously as a 0.3 M solution, tromethamine act as a proton acceptor and prevents or corrects acidosis by actively binding hydrogen ions (H + ). It binds not only cations of fixed or metabolic acids, but also hydrogen ions of carbonic acid, thus increasing bicarbonate anion (HCO 3 – ). Tromethamine also acts as an osmotic diuretic, increasing urine flow, urinary pH, and excretion of fixed acids, carbon dioxide and electrolytes. A significant fraction of tromethamine (30% at pH 7.40) is not ionized and therefore is capable of reaching equilibrium in total body water. This portion may penetrate cells and may neutralize acidic ions of the intracellular fluid.
The drug is rapidly eliminated by the kidney; 75% or more appears in the urine after eight hours. Urinary excretion continues over a period of three days.
Water is an essential constituent of all body tissues and accounts for approximately 70% of total body weight. Average normal adult daily requirement ranges from two to three liters (1.0 to 1.5 liters each for insensible water loss by perspiration and urine production).
Water balance is maintained by various regulatory mechanisms. Water distribution depends primarily on the concentration of electrolytes in the body compartments and sodium (Na + ) plays a major role in maintaining physiologic equilibrium.
HOW SUPPLIED
Tromethamine Injection is available as:
Unit of Sale | Concentration | Each |
NDC 71357-001-06 | NDC 71357-001-01 | |
Case of 6 Single-dose 500 mL large volume glass containers | 500 mL (150 mEq) | 1 Single-dose 500 mL large volume glass container |
Store at 20 to 25°C (68 to 77°F). [See USP Controlled Room Temperature.]
Protect from freezing.
Revised: June, 2024
Distributed by:
Milla Pharmaceuticals Inc.,
an A.forall company
White Bear Lake
MN 55110
USA
Made in Italy