Get your patient on Terconazole - Terconazole suppository (Terconazole)
Terconazole - Terconazole suppository prescribing information
INDICATIONS AND USAGE
Terconazole Vaginal Suppositories, 80 mg is indicated for the local treatment of vulvovaginal candidiasis (moniliasis). As this product is effective only for vulvovaginitis caused by the genus Candida , the diagnosis should be confirmed by KOH smears and/or cultures.
DOSAGE AND ADMINISTRATION
One Terconazole Vaginal Suppository (80 mg terconazole) should be administered intravaginally once daily at bedtime for three consecutive days.
Before prescribing another course of therapy, the diagnosis should be reconfirmed by smears and/or cultures and other pathogens commonly associated with vulvovaginitis ruled out. The therapeutic effect of terconazole vaginal suppositories is not affected by menstruation.
CONTRAINDICATIONS
Patients known to be hypersensitive to terconazole or to any of the components of the suppositories.
ADVERSE REACTIONS
Adverse Reactions from Clinical Trials
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
During controlled clinical studies conducted in the United States, 284 patients with vulvovaginal candidiasis were treated with terconazole 80 mg vaginal suppositories. Based on comparative analyses with placebo (295 patients), the adverse experiences considered adverse reactions most likely related to terconazole 80 mg vaginal suppositories were headache (30.3% vs. 20.7% with placebo) and pain of the female genitalia (4.2% vs. 0.7% with placebo). Adverse reactions that have also been reported but were not statistically significantly different from placebo were burning (15.2% vs. 11.2% with placebo) and body pain (3.9% vs. 1.7% with placebo). Fever (2.8% vs. 1.4% with placebo) and chills (1.8% vs. 0.7% with placebo) have also been reported. The adverse drug experience on terconazole most frequently causing discontinuation was burning (2.5% vs. 1.4% with placebo) and pruritus (1.8% vs. 1.4% with placebo).
Post-marketing Experience
The following adverse drug reactions have been first identified during post-marketing experience with terconazole:. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
General: Asthenia, Influenza-Like Illness consisting of multiple listed reactions including fever and chills, nausea, vomiting, myalgia, arthralgia, malaise
Immune: Hypersensitivity, Anaphylaxis, Face Edema
Nervous: Dizziness
Respiratory: Bronchospasm
Skin: Rash, Toxic Epidermal Necrolysis, Urticaria
Drug Interactions
The therapeutic effect of this product is not affected by oral contraceptive usage.
DESCRIPTION
Terconazole Vaginal Suppositories are white to off-white suppositories for intravaginal administration containing 80 mg of the antifungal agent terconazole, cis -1-[ p -[[2-(2,4-Dichlorophenyl)-2-(1 H -1,2,4-triazol-1-ylmethyl)-1,3-dioxolan-4-yl]methoxy]phenyl]-4-isopropylpiperazine, in triglycerides derived from coconut and/or palm kernel oil (a base of hydrogenated vegetable oils) and butylated hydroxyanisole.
The structural formula of terconazole is as follows:
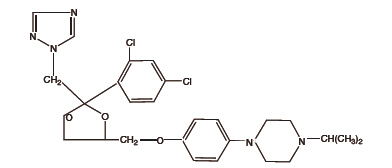 | TERCONAZOLE C 26 H 31 Cl 2 N 5 O 3 |
Terconazole, a triazole derivative, is a white to almost white powder with a molecular weight of 532.47. It is insoluble in water; sparingly soluble in ethanol; and soluble in butanol.
CLINICAL PHARMACOLOGY
Absorption
Following a single intravaginal application of a suppository containing 240 mg 14 C-terconazole to healthy women, approximately 70% (range: 64 to 76%) of terconazole remains in the vaginal area during the suppository retention period (16 hours); approximately 10% (range: 5 to 16%) of the administered radioactivity was absorbed systemically over 7 days. Maximum plasma concentrations of terconazole occur 5 to 10 hours after intravaginal application of the cream or suppository. Systemic exposure to terconazole is approximately proportional to the applied dose, whether as the cream or suppository. The rate and extent of absorption of terconazole are similar in patients with vulvovaginal candidiasis (pregnant or non-pregnant) and healthy subjects.
Distribution
Terconazole is highly protein bound (94.9%) in human plasma and the degree of binding is independent of drug concentration over the range of 0.01 to 5 mcg/mL.
Metabolism
Systemically absorbed terconazole is extensively metabolized (>95%).
Elimination
Across various studies in healthy women, after single or multiple intravaginal administration of terconazole as the cream or suppository/ovule, the mean elimination half-life of unchanged terconazole ranged from 6.4 to 8.5 hours. Following a single intravaginal administration of a suppository containing 240 mg 14 C-terconazole to hysterectomized or tubal ligated women, approximately 3 to 10% (mean ± SD: 5.7 ± 3%) of the administered radioactivity was eliminated in the urine and 2 to 6% (mean ± SD: 4.2 ± 1.6%) was eliminated in the feces during the 7-day collection period.
Multiple Dosing
There is no significant increase in maximum plasma concentration or overall exposure (AUC) after multiple daily applications of the cream for 7 days or suppositories for 3 days.
Photosensitivity reactions were observed in some normal volunteers following repeated dermal application of terconazole 2% and 0.8% creams under conditions of filtered artificial ultraviolet light.
Photosensitivity reactions have not been observed in U.S. and foreign clinical trials in patients who were treated with terconazole suppositories or vaginal cream (0.4% and 0.8%).
Microbiology
Mechanism of action
Terconazole, an azole antifungal agent, inhibits fungal cytochrome P-450-mediated 14 alpha-lanosterol demethylase enzyme. This enzyme functions to convert lanosterol to ergosterol. The accumulation of 14 alpha-methyl sterols correlates with the subsequent loss of ergosterol in the fungal cell wall and may be responsible for the antifungal activity of terconazole. Mammalian cell demethylation is less sensitive to terconazole inhibition.
Activity in vitro
Terconazole exhibits antifungal activity in vitro against Candida albicans and other Candida species. The MIC values of terconazole against most Lactobacillus spp. typically found in the human vagina were ≥128 mcg/mL; therefore these beneficial bacteria are not affected by drug treatment.
Adverse Reactions from Clinical Trials
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
During controlled clinical studies conducted in the United States, 284 patients with vulvovaginal candidiasis were treated with terconazole 80 mg vaginal suppositories. Based on comparative analyses with placebo (295 patients), the adverse experiences considered adverse reactions most likely related to terconazole 80 mg vaginal suppositories were headache (30.3% vs. 20.7% with placebo) and pain of the female genitalia (4.2% vs. 0.7% with placebo). Adverse reactions that have also been reported but were not statistically significantly different from placebo were burning (15.2% vs. 11.2% with placebo) and body pain (3.9% vs. 1.7% with placebo). Fever (2.8% vs. 1.4% with placebo) and chills (1.8% vs. 0.7% with placebo) have also been reported. The adverse drug experience on terconazole most frequently causing discontinuation was burning (2.5% vs. 1.4% with placebo) and pruritus (1.8% vs. 1.4% with placebo).
HOW SUPPLIED
Terconazole Vaginal Suppositories 80 mg are available as 2.5 g, elliptically-shaped white to off-white suppositories in packages of three with a vaginal applicator. NDC 51672-1330-3
Store at 20°- 25°C (68°- 77°F) [see USP Controlled Room Temperature].
Mechanism of action
Terconazole, an azole antifungal agent, inhibits fungal cytochrome P-450-mediated 14 alpha-lanosterol demethylase enzyme. This enzyme functions to convert lanosterol to ergosterol. The accumulation of 14 alpha-methyl sterols correlates with the subsequent loss of ergosterol in the fungal cell wall and may be responsible for the antifungal activity of terconazole. Mammalian cell demethylation is less sensitive to terconazole inhibition.