Get your patient on Tarina Fe 1/20 Eq - Norethindrone Acetate And Ethinyl Estradiol And Ferrous Fumarate (Norethindrone Acetate And Ethinyl Estradiol And Ferrous Fumarate)
Tarina Fe 1/20 Eq - Norethindrone Acetate And Ethinyl Estradiol And Ferrous Fumarate prescribing information
INDICATIONS AND USAGE
Tarina Fe 1/20 EQ is indicated for the prevention of pregnancy in women who elect to use oral contraceptives as a method of contraception. Oral contraceptives are highly effective. Table I lists the typical accidental pregnancy rates for users of combination oral contraceptives and other methods of contraception. The efficacy of these contraceptive methods, except sterilization, depends upon the reliability with which they are used. Correct and consistent use of methods can result in lower failure rates.
| TABLE 1 LOWEST EXPECTED AND TYPICAL FAILURE RATES DURING THE FIRST YEAR OF CONTINUOUS USE OF A METHOD | ||
| % of Women Experiencing an Unintended Pregnancy in the First Year of Continuous Use | ||
| Method | Lowest Expected• | Typical•• |
| (No contraception) | (85) | (85) |
| Oral contraceptives | 3 | |
| combined | 0.1 | N/A••• |
| progestin only | 0.5 | N/A••• |
| Diaphragm with spermicidal cream or jelly | 6 | 20 |
| Spermicides alone (foam, creams, gels, vaginal suppositories, and vaginal film) | 6 | 26 |
| Vaginal Sponge | ||
| nulliparous | 9 | 20 |
| parous | 20 | 40 |
| Implant | 0.05 | 0.05 |
| Injection: depot medroxyprogesterone acetate | 0.3 | 0.3 |
| IUD | ||
| progesterone T | 1.5 | 2 |
| copper T 380A | 0.6 | 0.8 |
| LNg 20 | 0.1 | 0.1 |
| Condom without spermicides | ||
| female | 5 | 21 |
| male | 3 | 14 |
| Cervical Cap with spermicidal cream or jelly | ||
| nulliparous | 9 | 20 |
| parous | 26 | 40 |
| Periodic abstinence (all methods) | 1 to 9 | 25 |
| Withdrawal | 4 | 19 |
| Female sterilization | 0.5 | 0.5 |
| Male sterilization | 0.1 | 0.15 |
| Adapted from RA Hatcher et al, Reference 7. • The authors’ best guess of the percentage of women expected to experience an accidental pregnancy among couples who initiate a method (not necessarily for the first time) and who use it consistently and correctly during the first year if they do not stop for any other reason. •• This term represents “typical” couples who initiate use of a method (not necessarily for the first time), who experience an accidental pregnancy during the first year if they do not stop use for any other reason. ••• N/A--Data not available. | ||
DOSAGE AND ADMINISTRATION
The blister pack has been designed to make oral contraceptive dosing as easy and as convenient as possible. The tablets are arranged in four rows of seven tablets each, with the days of the week appearing on the blister pack above the first row of tablets.
Note: Each blister pack has been preprinted with the days of the week, starting with Sunday, to facilitate a Sunday-Start regimen. Six different day label stickers have been provided with the Detailed Patient & Brief Summary Patient Package Insert in order to accommodate a Day-1 Start regimen. If the patient is using the Day-1 Start regimen, she should place the self-adhesive day label sticker that corresponds to her starting day over the preprinted days.
Important: The patient should be instructed to use an additional method of protection until after the first week of administration in the initial cycle when utilizing the Sunday-Start regimen.
The possibility of ovulation and conception prior to initiation of use should be considered. Dosage and Administration for 28-Day Dosage Regimen To achieve maximum contraceptive effectiveness, Tarina Fe 1/20 EQ should be taken exactly as directed and at intervals not exceeding 24 hours.
Tarina Fe 1/20 EQ provides a continuous administration regimen consisting of 21 light yellow to yellow tablets of norethindrone acetate and ethinyl estradiol and 7 brown non-hormone containing tablets of ferrous fumarate. The ferrous fumarate tablets are present to facilitate ease of drug administration via a 28-day regimen and do not serve any therapeutic purpose. There is no need for the patient to count days between cycles because there are no “off-tablet days.”
A. Sunday-Start Regimen: The patient begins taking the first light yellow to yellow tablet from the top row of the blister pack (labeled Sunday) on the first Sunday after menstrual flow begins. When the menstrual flow begins on Sunday, the first light yellow to yellow tablet is taken on the same day. The patient takes one light yellow to yellow tablet daily for 21 days. The last light yellow to yellow tablet in the blister pack will be taken on a Saturday. Upon completion of all 21 light yellow to yellow tablets, and without interruption, the patient takes one brown tablet daily for 7 days. Upon completion of this first course of tablets, the patient begins a second course of 28-day tablets, without interruption, the next day (Sunday), starting with the Sunday light yellow to yellow tablet in the top row. Adhering to this regimen of one light yellow to yellow tablet daily for 21 days, followed without interruption by one brown tablet daily for seven days, the patient will start all subsequent cycles on a Sunday.
B. Day-1 Start Regimen: The first day of menstrual flow is Day 1. The patient places the self-adhesive day label sticker that corresponds to her starting day over the preprinted days on the blister pack. She starts taking one light yellow to yellow tablet daily, beginning with the first light yellow to yellow tablet in the top row. After the last light yellow to yellow tablet (at the end of the third row) has been taken, the patient will then take the brown tablets for a week (7 days). For all subsequent cycles, the patient begins a new 28 tablet regimen on the eighth day after taking her last light yellow to yellow tablet, again starting with the first tablet in the top row after placing the appropriate day label sticker over the preprinted days on the blister pack. Following this regimen of 21 light yellow to yellow tablets and 7 brown tablets, the patient will start all subsequent cycles on the same day of the week as the first course.
Tablets should be taken regularly with a meal or at bedtime. It should be stressed that efficacy of medication depends on strict adherence to the dosage schedule.
Special Notes on Administration
Menstruation usually begins two or three days, but may begin as late as the fourth or fifth day, after the brown tablets have been started. In any event, the next course of tablets should be started without interruption. If spotting occurs while the patient is taking light yellow to yellow tablets, continue medication without interruption.
If the patient forgets to take one or more light yellow to yellow tablets, the following is suggested:
One tablet is missed
- take tablet as soon as remembered
- take next tablet at the regular time
Two consecutive tablets are missed (week 1 or week 2)
- take two tablets as soon as remembered
- take two tablets the next day
- use another birth control method for seven days following the missed tablets
Two consecutive tablets are missed (week 3)
Sunday-Start Regimen
- take one tablet daily until Sunday
- discard remaining tablets
- start new pack of tablets immediately (Sunday)
- use another birth control method for seven days following the missed tablets
Day-1 Start Regimen
- discard remaining tablets
- start new pack of tablets that same day
- use another birth control method for seven days following the missed tablets
Three (or more) consecutive tablets are missed
Sunday-Start Regimen
- take one tablet daily until Sunday
- discard remaining tablets
- start new pack of tablets immediately (Sunday)
- use another birth control method for seven days following the missed tablets
Day-1 Start Regimen
- discard remaining tablets
- start new pack of tablets that same day
- use another birth control method for seven days following the missed tablets
The possibility of ovulation occurring increases with each successive day that scheduled light yellow to yellow tablets are missed. While there is little likelihood of ovulation occurring if only one light yellow to yellow tablet is missed, the possibility of spotting or bleeding is increased. This is particularly likely to occur if two or more consecutive light yellow to yellow tablets are missed.
If the patient forgets to take any of the seven brown tablets in week four, those brown tablets that were missed are discarded and one brown tablet is taken each day until the pack is empty. A back-up birth control method is not required during this time. A new pack of tablets should be started no later than the eighth day after the last light yellow to yellow tablet was taken.
In the rare case of bleeding which resembles menstruation, the patient should be advised to discontinue medication and then begin taking tablets from a new blister pack on the next Sunday or the first day (Day-1), depending on her regimen. Persistent bleeding which is not controlled by this method indicates the need for reexamination of the patient, at which time nonfunctional causes should be considered.
Use of Oral Contraceptives in the Event of a Missed Menstrual Period
1. If the patient has not adhered to the prescribed dosage regimen, the possibility of pregnancy should be considered after the first missed period and oral contraceptives should be withheld until pregnancy has been ruled out.
2. If the patient has adhered to the prescribed regimen and misses two consecutive periods, pregnancy should be ruled out before continuing the contraceptive regimen.
After several months on treatment, bleeding may be reduced to a point of virtual absence. This reduced flow may occur as a result of medication, in which event it is not indicative of pregnancy.
CONTRAINDICATIONS
Oral contraceptives are contraindicated in women who currently have the following conditions:
- Thrombophlebitis or thromboembolic disorders
- A past history of deep vein thrombophlebitis or thromboembolic disorders
- Cerebral vascular or coronary artery disease
- Current diagnosis of, or history of, breast cancer, which may be hormone sensitive
- Carcinoma of the endometrium or other known or suspected estrogen-dependent neoplasia
- Undiagnosed abnormal genital bleeding
- Cholestatic jaundice of pregnancy or jaundice with prior pill use
- Hepatic adenomas or carcinomas
- Are receiving Hepatitis C drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to the potential for ALT elevations (see WARNINGS, Risk of Liver Enzyme Elevations with Concomitant Hepatitis C Treatment ) .
ADVERSE REACTIONS
An increased risk of the following serious adverse reactions has been associated with the use of oral contraceptives (see WARNINGS section):
- Thrombophlebitis
- Arterial thromboembolism
- Pulmonary embolism
- Myocardial infarction
- Cerebral hemorrhage
- Cerebral thrombosis
- Hypertension
- Gallbladder disease
- Hepatic adenomas or benign liver tumors
Post Marketing Experience
Five studies that compared breast cancer risk between ever-users (current or past use) of COCs and never-users of COCs reported no association between ever use of COCs and breast cancer risk, with effect estimates ranging from 0.90 to 1.12 (Figure 1) (70 to 74).
Three studies compared breast cancer risk between current or recent COC users (<6 months since last use) and never users of COCs (Figure 1) (70,73,75). One of these studies reported no association between breast cancer risk and COC use. The other two studies found an increased relative risk of 1.19 to 1.33 with current or recent use. Both of these studies found an increased risk of breast cancer with current use of longer duration, with relative risks ranging from 1.03 with less than one year of COC use to approximately 1.4 with more than 8 to 10 years of COC use.
FIGURE 1: RELEVANT STUDIES OF RISK OF BREAST CANCER WITH COMBINED ORAL CONTRACEPTIVES
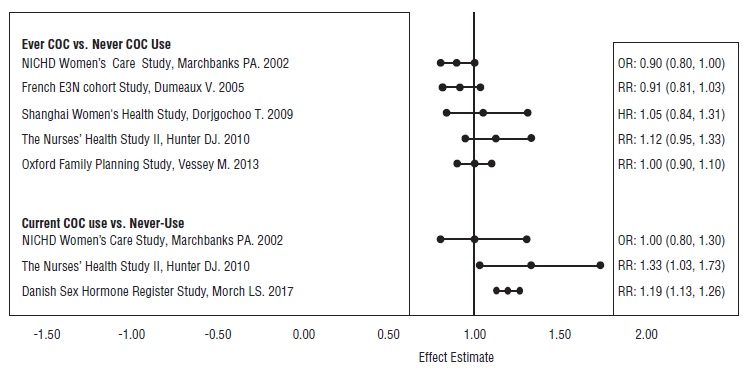
RR = relative risk; OR = odds ratio; HR = hazard ratio. “ever COC” are females with current or past COC use; “never COC use” are females that never used COCs.
There is evidence of an association between the following conditions and the use of oral contraceptives, although additional confirmatory studies are needed:
- Mesenteric thrombosis
- Retinal thrombosis
The following adverse reactions have been reported in patients receiving oral contraceptives and are believed to be drug-related:
- Nausea
- Vomiting
- Gastrointestinal symptoms (such as abdominal cramps and bloating)
- Breakthrough bleeding
- Spotting
- Change in menstrual flow
- Amenorrhea
- Temporary infertility after discontinuation of treatment
- Edema
- Melasma which may persist
- Breast changes: tenderness, enlargement, secretion
- Change in weight (increase or decrease)
- Change in cervical erosion and secretion
- Diminution in lactation when given immediately postpartum
- Cholestatic jaundice
- Migraine
- Rash (allergic)
- Depression
- Reduced tolerance to carbohydrates
- Vaginal candidiasis
- Change in corneal curvature (steepening)
- Intolerance to contact lenses
The following adverse reactions have been reported in users of oral contraceptives and the association has been neither confirmed nor refuted:
- Pre-menstrual syndrome
- Cataracts
- Changes in appetite
- Cystitis-like syndrome
- Headache
- Nervousness
- Dizziness
- Hirsutism
- Loss of scalp hair
- Erythema multiforme
- Erythema nodosum
- Hemorrhagic eruption
- Vaginitis
- Porphyria
- Impaired renal function
- Hemolytic uremic syndrome
- Budd-Chiari syndrome
- Acne
- Changes in libido
- Colitis
Drug Interactions
Effects of Other Drugs on Oral Contraceptives (69)
Rifampin: Metabolism of both norethindrone and ethinyl estradiol is increased by rifampin. A reduction in contraceptive effectiveness and increased incidence of breakthrough bleeding and menstrual irregularities have been associated with concomitant use of rifampin.
Anticonvulsants : Anticonvulsants such as phenobarbital, phenytoin, and carbamazepine, have been shown to increase the metabolism of ethinyl estradiol and/or norethindrone, which could result in a reduction in contraceptive effectiveness.
Troglitazone: Administration of troglitazone with an oral contraceptive containing ethinyl estradiol and norethindrone reduced the plasma concentrations of both by approximately 30%, which could result in a reduction in contraceptive effectiveness.
Antibiotics: Pregnancy while taking oral contraceptives has been reported when the oral contraceptives were administered with antimicrobials such as ampicillin, tetracycline, and griseofulvin. However, clinical pharmacokinetic studies have not demonstrated any consistent effect of antibiotics (other than rifampin) on plasma concentrations of synthetic steroids.
Atorvastatin: Coadministration of atorvastatin and an oral contraceptive increased AUC values for norethindrone and ethinyl estradiol by approximately 30% and 20%, respectively.
Concomitant Use with HCV Combination Therapy – Liver Enzyme Elevation
Co-administration of Tarina Fe 1/20 EQ with HCV drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir is contraindicated due to potential for ALT elevations (see WARNINGS, Risk of Liver Enzyme Elevations with concomitant Hepatitis C Treatment ). Co-administration of Tarina Fe 1/20 EQ and glecaprevir/pibrentasvir is not recommended due to potential for ALT elevations.
Other: Ascorbic acid and acetaminophen may increase plasma ethinyl estradiol concentrations, possibly by inhibition of conjugation. A reduction in contraceptive effectiveness and increased incidence of breakthrough bleeding has been suggested with phenylbutazone.
Effects of Oral Contraceptives on Other Drugs
Oral contraceptive combinations containing ethinyl estradiol may inhibit the metabolism of other compounds. Increased plasma concentrations of cyclosporine, prednisolone, and theophylline have been reported with concomitant administration of oral contraceptives. In addition, oral contraceptives may induce the conjugation of other compounds. Decreased plasma concentrations of acetaminophen and increased clearance of temazepam, salicylic acid, morphine, and clofibric acid have been noted when these drugs were administered with oral contraceptives.
DESCRIPTION
Tarina Fe 1/20 EQ is progestogen-estrogen combination. Tarina Fe 1/20 EQ: Each provides a continuous dosage regimen consisting of 21 oral contraceptive tablets and seven ferrous fumarate tablets. The ferrous fumarate tablets are present to facilitate ease of drug administration via a 28-day regimen, are non-hormonal, and do not serve any therapeutic purpose. Each light yellow to yellow tablet contains norethindrone acetate USP (17 alpha-ethinyl-19-nortestosterone acetate), 1 mg; ethinyl estradiol USP (17 alpha-ethinyl-1,3,5(10)-estratriene-3, 17 beta-diol), 20 mcg. Each light yellow to yellow tablet contains the following inactive ingredients: compressible sugar, croscarmellose sodium, D&C yellow No.10 aluminum lake, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, and vitamin E. Each brown placebo tablet contains the following ingredients: croscarmellose sodium, ferrous fumarate, lactose monohydrate, magnesium stearate, microcrystalline cellulose, Nat spearmint FL, povidone and sucralose. The ferrous fumarate tablets do not serve any therapeutic purpose. The structural formulas are as follows:
Meets USP Dissolution Test 2
CLINICAL PHARMACOLOGY
Combination oral contraceptives act by suppression of gonadotropins. Although the primary mechanism of this action is inhibition of ovulation, other alterations include changes in the cervical mucus (which increase the difficulty of sperm entry into the uterus) and the endometrium (which reduce the likelihood of implantation). Pharmacokinetics The pharmacokinetics of Tarina Fe 1/20 EQ has not been characterized; however, the following pharmacokinetic information regarding norethindrone acetate and ethinyl estradiol is taken from the literature. Absorption Norethindrone acetate appears to be completely and rapidly deacetylated to norethindrone after oral administration, since the disposition of norethindrone acetate is indistinguishable from that of orally administered norethindrone (1). Norethindrone acetate and ethinyl estradiol are subject to first-pass metabolism after oral dosing, resulting in an absolute bioavailability of approximately 64% for norethindrone and 43% for ethinyl estradiol (1 to 3). Distribution Volume of distribution of norethindrone and ethinyl estradiol ranges from 2 to 4 L/kg (1 to 3). Plasma protein binding of both steroids is extensive (greater than 95%); norethindrone binds to both albumin and sex hormone binding globulin, whereas ethinyl estradiol binds only to albumin (4). Metabolism Norethindrone undergoes extensive biotransformation, primarily via reduction, followed by sulfate and glucuronide conjugation. The majority of metabolites in the circulation are sulfates, with glucuronides accounting for most of the urinary metabolites (5). A small amount of norethindrone acetate is metabolically converted to ethinyl estradiol. Ethinyl estradiol is also extensively metabolized, both by oxidation and by conjugation with sulfate and glucuronide. Sulfates are the major circulating conjugates of ethinyl estradiol and glucuronides predominate in urine. The primary oxidative metabolite is 2-hydroxy ethinyl estradiol, formed by the CYP3A4 isoform of cytochrome P450. Part of the first-pass metabolism of ethinyl estradiol is believed to occur in gastrointestinal mucosa. Ethinyl estradiol may undergo enterohepatic circulation (6). Excretion Norethindrone and ethinyl estradiol are excreted in both urine and feces, primarily as metabolites (5, 6). Plasma clearance values for norethindrone and ethinyl estradiol are similar (approximately 0.4 L/hr/kg) (1 to 3). Special Population Race The effect of race on the disposition of Tarina Fe 1/20 EQ has not been evaluated. Renal Insufficiency The effect of renal disease on the disposition of Tarina Fe 1/20 EQ has not been evaluated. In premenopausal women with chronic renal failure undergoing peritoneal dialysis who received multiple doses of an oral contraceptive containing ethinyl estradiol and norethindrone, plasma ethinyl estradiol concentrations were higher and norethindrone concentrations were unchanged compared to concentrations in premenopausal women with normal renal function. Hepatic Insufficiency The effect of hepatic disease on the disposition of Tarina Fe 1/20 EQ has not been evaluated. However, ethinyl estradiol and norethindrone may be poorly metabolized in patients with impaired liver function. Drug-Drug Interactions Numerous drug-drug interactions have been reported for oral contraceptives. A summary of these is found under PRECAUTIONS , Drug Interactions .
HOW SUPPLIED
Tarina Fe 1/20 EQ ® (norethindrone acetate and ethinyl estradiol tablets USP, 1 mg/20 mcg and ferrous fumarate tablets, 75 mg) are light yellow to yellow, round, flat-faced, beveled-edge, uncoated tablets, debossed with ‘S’ on one side and ‘64’ on other side of the tablet. Each brown mottled, round, flat-faced beveled-edge tablet contains 75 mg ferrous fumarate and is debossed with ‘S’ on one side and ‘57’ on other side of the tablet. The ferrous fumarate tablets are present to facilitate ease of drug administration via a 28-day regimen, are non-hormonal, and do not serve any therapeutic purpose. 1 pouch of 28 tablets NDC 50102-228-21 Carton of 3 pouches NDC 50102-228-23 Store at 20 o to 25 o C (68 o to 77 o F) [see USP Controlled Room Temperature].