Get your patient on Nifedipine - Nifedipine tablet, Film Coated, Extended Release (Nifedipine)
Nifedipine - Nifedipine tablet, Film Coated, Extended Release prescribing information
INDICATIONS AND USAGE
I. Vasospastic Angina Nifedipine Extended-Release Tablets, USP are indicated for the management of vasospastic angina confirmed by any of the following criteria: 1) classical pattern of angina at rest accompanied by ST segment elevation, 2) angina or coronary artery spasm provoked by ergonovine, or 3) angiographically demonstrated coronary artery spasm. In those patients who have had angiography, the presence of significant fixed obstructive disease is not incompatible with the diagnosis of vasospastic angina, provided that the above criteria are satisfied. Nifedipine Extended-Release Tablets, USP may also be used where the clinical presentation suggests a possible vasospastic component, but where vasospasm has not been confirmed, e.g., where pain has a variable threshold on exertion, or in unstable angina where electrocardiographic findings are compatible with intermittent vasospasm, or when angina is refractory to nitrates and/or adequate doses of beta blockers.
II. Chronic Stable Angina (Classical Effort-Associated Angina) Nifedipine Extended-Release Tablets, USP are indicated for the management of chronic stable angina (effort-associated angina) without evidence of vasospasm in patients who remain symptomatic despite adequate doses of beta blockers and/or organic nitrates or who cannot tolerate those agents.
In chronic stable angina (effort-associated angina), nifedipine has been effective in controlled trials of up to eight weeks duration in reducing angina frequency and increasing exercise tolerance, but confirmation of sustained effectiveness and evaluation of long-term safety in these patients is incomplete.
Controlled studies in small numbers of patients suggest concomitant use of nifedipine and beta-blocking agents may be beneficial in patients with chronic stable angina, but available information is not sufficient to predict with confidence the effects of concurrent treatment, especially in patients with compromised left ventricular function or cardiac conduction abnormalities. When introducing such concomitant therapy, care must be taken to monitor blood pressure closely, since severe hypotension can occur from the combined effects of the drugs (see WARNINGS ).
III. Hypertension Nifedipine Extended-Release Tablets, USP are indicated for the treatment of hypertension, to lower blood pressure. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions. These benefits have been seen in controlled trials of antihypertensive drugs from a wide variety of pharmacologic classes including Nifedipine Extended-Release Tablets, USP.
Control of high blood pressure should be part of comprehensive cardiovascular risk management, including, as appropriate, lipid control, diabetes management, antithrombotic therapy, smoking cessation, exercise, and limited sodium intake. Many patients will require more than one drug to achieve blood pressure goals. For specific advice on goals and management, see published guidelines, such as those of the National High Blood Pressure Education Program’s Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC).
Numerous antihypertensive drugs, from a variety of pharmacologic classes and with different mechanisms of action, have been shown in randomized controlled trials to reduce cardiovascular morbidity and mortality, and it can be concluded that it is blood pressure reduction, and not some other pharmacologic property of the drugs, that is largely responsible for those benefits. The largest and most consistent cardiovascular outcome benefit has been a reduction in the risk of stroke, but reductions in myocardial infarction and cardiovascular mortality also have been seen regularly.
Elevated systolic or diastolic pressure causes increased cardiovascular risk, and the absolute risk increase per mmHg is greater at higher blood pressures, so that even modest reductions of severe hypertension can provide substantial benefit. Relative risk reduction from blood pressure reduction is similar across populations with varying absolute risk, so the absolute benefit is greater in patients who are at higher risk independent of their hypertension (for example, patients with diabetes or hyperlipidemia), and such patients would be expected to benefit from more aggressive treatment to a lower blood pressure goal.
Some antihypertensive drugs have smaller blood pressure effects (as monotherapy) in black patients, and many antihypertensive drugs have additional approved indications and effects (e.g., on angina, heart failure, or diabetic kidney disease). These considerations may guide selection of therapy.
Nifedipine Extended-Release Tablets, USP may be used alone or in combination with other antihypertensive agents.
DOSAGE AND ADMINISTRATION
Dosage must be adjusted according to each patient’s needs. Therapy for either hypertension or angina should be initiated with 30 or 60 mg once daily. Nifedipine Extended-Release Tablets, USP should be swallowed whole and should not be bitten or divided. In general, titration should proceed over a 7–14 day period so that the physician can fully assess the response to each dose level and monitor blood pressure before proceeding to higher doses. Since steady-state plasma levels are achieved on the second day of dosing, titration may proceed more rapidly, if symptoms so warrant, provided the patient is assessed frequently. Titration to doses above 120 mg are not recommended.
Angina patients controlled on nifedipine capsules alone or in combination with other antianginal medications may be safely switched to Nifedipine Extended-Release Tablets, USP at the nearest equivalent total daily dose (e.g., 30 mg t.i.d. of nifedipine capsules may be changed to 90 mg once daily of Nifedipine Extended-Release Tablets, USP). Subsequent titration to higher or lower doses may be necessary and should be initiated as clinically warranted. Experience with doses greater than 90 mg in patients with angina is limited. Therefore, doses greater than 90 mg should be used with caution and only when clinically warranted.
Avoid co-administration of nifedipine with grapefruit juice (see CLINICAL PHARMACOLOGY and PRECAUTIONS: Other Interactions ).
No “rebound effect” has been observed upon discontinuation of nifedipine extended-release tablets. However, if discontinuation of nifedipine is necessary, sound clinical practice suggests that the dosage should be decreased gradually with close physician supervision.
Care should be taken when dispensing Nifedipine Extended-Release Tablets, USP to assure that the extended-release dosage form has been prescribed.
CONTRAINDICATIONS
Known hypersensitivity reaction to nifedipine.
ADVERSE EXPERIENCES
Over 1000 patients from both controlled and open trials with nifedipine extended-release tablets in hypertension and angina were included in the evaluation of adverse experiences. All side effects reported during nifedipine extended-release tablet therapy were tabulated independent of their causal relation to medication. The most common side effect reported with nifedipine extended-release tablet was edema which was dose related and ranged in frequency from approximately 10% to about 30% at the highest dose studied (180 mg). Other common adverse experiences reported in placebo-controlled trials include:
| Adverse Effect | Nifedipine Extended-Release Tablet (%) (N=707) | Placebo (%) (N=266) |
|---|---|---|
| Headache | 15.8 | 9.8 |
| Fatigue | 5.9 | 4.1 |
| Dizziness | 4.1 | 4.5 |
| Constipation | 3.3 | 2.3 |
| Nausea | 3.3 | 1.9 |
Of these, only edema and headache were more common in nifedipine extended-release tablet patients than placebo patients.
The following adverse reactions occurred with an incidence of less than 3.0%. With the exception of leg cramps, the incidence of these side effects was similar to that of placebo alone.
Body as a Whole/Systemic: asthenia, flushing, pain Cardiovascular: palpitations Central Nervous System: insomnia, nervousness, paresthesia, somnolence Dermatologic: pruritus, rash Gastrointestinal: abdominal pain, diarrhea, dry mouth, dyspepsia, flatulence Musculoskeletal: arthralgia, leg cramps Respiratory: chest pain (nonspecific), dyspnea Urogenital: impotence, polyuria
Other adverse reactions were reported sporadically with an incidence of 1.0% or less. These include:
Body as a Whole/Systemic: face edema, fever, hot flashes, malaise, periorbital edema, rigors Cardiovascular: arrhythmia, hypotension, increased angina, tachycardia, syncope Central Nervous System: anxiety, ataxia, decreased libido, depression, hypertonia, hypoesthesia, migraine, paroniria, tremor, vertigo Dermatologic: alopecia, increased sweating, urticaria, purpura Gastrointestinal: eructation, gastroesophageal reflux, gum hyperplasia, melena, vomiting, weight increase Musculoskeletal: back pain, gout, myalgias Respiratory: coughing, epistaxis, upper respiratory tract infection, respiratory disorder, sinusitis Special Senses: abnormal lacrimation, abnormal vision, taste perversion, tinnitus Urogenital/Reproductive: breast pain, dysuria, hematuria, nocturia
Adverse experiences which occurred in less than 1 in 1000 patients cannot be distinguished from concurrent disease states or medications.
The following adverse experiences, reported in less than 1% of patients, occurred under conditions (e.g., open trials, marketing experience) where a causal relationship is uncertain: gastrointestinal irritation, gastrointestinal bleeding, gynecomastia.
Gastrointestinal obstruction resulting in hospitalization and surgery, including the need for bezoar removal, has occurred in association with nifedipine extended-release tablet, even in patients with no prior history of gastrointestinal disease (see WARNINGS ).
Cases of tablet adherence to the gastrointestinal wall with ulceration have been reported, some requiring hospitalization and intervention.
In multiple-dose U.S. and foreign controlled studies with nifedipine capsules in which adverse reactions were reported spontaneously, adverse effects were frequent but generally not serious and rarely required discontinuation of therapy or dosage adjustment. Most were expected consequences of the vasodilator effects of nifedipine.
| NIFEDIPINE CAPSULES (%) | Placebo (%) | |
|---|---|---|
| Adverse Effect | (N=226) | (N=235) |
| Dizziness, lightheadedness, giddiness | 27 | 15 |
| Flushing, heat sensation | 25 | 8 |
| Headache | 23 | 20 |
| Weakness | 12 | 10 |
| Nausea, heartburn | 11 | 8 |
| Muscle cramps, tremor | 8 | 3 |
| Peripheral edema | 7 | 1 |
| Nervousness, mood changes | 7 | 4 |
| Palpitations | 7 | 5 |
| Dyspnea, cough, wheezing | 6 | 3 |
| Nasal congestion, sore throat | 6 | 8 |
There is also a large uncontrolled experience in over 2100 patients in the United States. Most of the patients had vasospastic or resistant angina pectoris, and about half had concomitant treatment with beta-adrenergic blocking agents. The relatively common adverse events were similar in nature to those seen with nifedipine extended-release tablet.
In addition, more serious adverse events were observed, not readily distinguishable from the natural history of the disease in these patients. It remains possible, however, that some or many of these events were drug related. Myocardial infarction occurred in about 4% of patients and congestive heart failure or pulmonary edema in about 2%. Ventricular arrhythmias or conduction disturbances each occurred in fewer than 0.5% of patients.
In a subgroup of over 1000 patients receiving nifedipine with concomitant beta blocker therapy, the pattern and incidence of adverse experiences was not different from that of the entire group of nifedipine-treated patients (see PRECAUTIONS ).
In a subgroup of approximately 250 patients with a diagnosis of congestive heart failure as well as angina, dizziness or lightheadedness, peripheral edema, headache, or flushing each occurred in one in eight patients. Hypotension occurred in about one in 20 patients. Syncope occurred in approximately one patient in 250. Myocardial infarction or symptoms of congestive heart failure each occurred in about one patient in 15. Atrial or ventricular dysrhythmias each occurred in about one patient in 150.
In post-marketing experience, there have been rare reports of exfoliative dermatitis caused by nifedipine. There have been rare reports of exfoliative or bullous skin adverse events (such as erythema multiforme, Stevens-Johnson Syndrome, and toxic epidermal necrolysis) and photosensitivity reactions. Acute generalized exanthematous pustulosis also has been reported.
Drug Interactions: Beta-adrenergic blocking agents: (see INDICATIONS AND USAGE and WARNINGS .) Experience in over 1400 patients with nifedipine capsules in a noncomparative clinical trial has shown that concomitant administration of nifedipine and beta-blocking agents is usually well tolerated, but there have been occasional literature reports suggesting that the combination may increase the likelihood of congestive heart failure, severe hypotension, or exacerbation of angina.
Long-acting Nitrates: Nifedipine may be safely co-administered with nitrates, but there have been no controlled studies to evaluate the antianginal effectiveness of this combination.
Digitalis: Administration of nifedipine with digoxin increased digoxin levels in nine of twelve normal volunteers. The average increase was 45%. Another investigator found no increase in digoxin levels in thirteen patients with coronary artery disease. In an uncontrolled study of over two hundred patients with congestive heart failure during which digoxin blood levels were not measured, digitalis toxicity was not observed. Since there have been isolated reports of patients with elevated digoxin levels, it is recommended that digoxin levels be monitored when initiating, adjusting, and discontinuing nifedipine to avoid possible over- or under-digitalization.
Coumarin Anticoagulants: There have been rare reports of increased prothrombin time in patients taking coumarin anticoagulants to whom nifedipine was administered. However, the relationship to nifedipine therapy is uncertain.
Cimetidine: A study in six healthy volunteers has shown a significant increase in peak nifedipine plasma levels (80%) and area-under-the-curve (74%), after a one week course of cimetidine at 1000 mg per day and nifedipine at 40 mg per day. Ranitidine produced smaller, non-significant increases. The effect may be mediated by the known inhibition of cimetidine on hepatic cytochrome P-450, the enzyme system probably responsible for the first-pass metabolism of nifedipine. If nifedipine therapy is initiated in a patient currently receiving cimetidine, cautious titration is advised.
Nifedipine is metabolized by CYP3A4. Co-administration of nifedipine with phenytoin, an inducer of CYP3A4, lowers the systemic exposure to nifedipine by approximately 70%. Avoid co-administration of nifedipine with phenytoin or any known CYP3A4 inducer or consider an alternative antihypertensive therapy.
CYP3A inhibitors such as fluconazole, itraconazole, clarithromycin, erythromycin, nefazodone, fluoxetine, saquinavir, indinavir, and nelfinavir may result in increased exposure to nifedipine when co-administered. Careful monitoring and dose adjustment may be necessary; consider initiating nifedipine at the lowest dose available if given concomitantly with these medications.
DESCRIPTION
Nifedipine is a drug belonging to a class of pharmacological agents known as the calcium channel blockers. Nifedipine is 3,5-pyridinedicarboxylic acid, 1,4-dihydro-2,6-dimethyl-4-(2-nitrophenyl)-, dimethyl ester, C 17 H 18 N 2 O 6 , and has the structural formula:
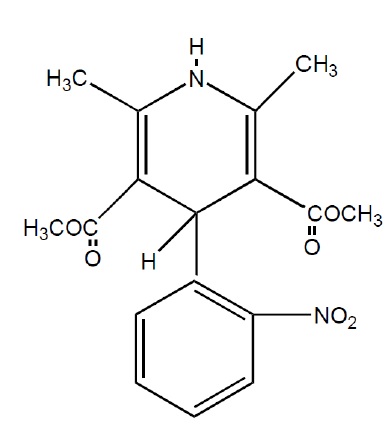
Nifedipine is a yellow crystalline substance, practically insoluble in water but soluble in ethanol. It has a molecular weight of 346.3. Nifedipine GITS (Gastrointestinal Therapeutic System) Tablet is formulated as a once-a-day controlled-release tablet for oral administration designed to deliver 90 mg of nifedipine.
Inert ingredients in the formulations are: black iron oxide, cellulose acetate, hypromellose, lactose monohydrate, polyethylene glycol, polyethylene oxide, povidone, propylene glycol, red iron oxide, shellac glaze, sodium chloride, stearic acid, titanium dioxide, triacetin.
System Components and Performance
Nifedipine Extended-Release Tablets, USP are similar in appearance to a conventional tablet. It consists, however, of a semipermeable membrane surrounding an osmotically active drug core. The core itself is divided into two layers: an “active” layer containing the drug, and a “push” layer containing pharmacologically inert (but osmotically active) components. As water from the gastrointestinal tract enters the tablet, pressure increases in the osmotic layer and “pushes” against the drug layer, releasing drug through the precision laser-drilled tablet orifice in the active layer.
Nifedipine Extended-Release Tablets, USP are designed to provide nifedipine at an approximately constant rate over 24 hours. This controlled rate of drug delivery into the gastrointestinal lumen is independent of pH or gastrointestinal motility. Nifedipine Extended-Release Tablets, USP depends for its action on the existence of an osmotic gradient between the contents of the bi-layer core and fluid in the gastrointestinal tract. Drug delivery is essentially constant as long as the osmotic gradient remains constant, and then gradually falls to zero. Upon swallowing, the biologically inert components of the tablet remain intact during gastrointestinal transit and are eliminated in the feces as an insoluble shell.
FDA approved dissolution test specifications differ from USP.
CLINICAL PHARMACOLOGY
Nifedipine is a calcium ion influx inhibitor (slow-channel blocker or calcium ion antagonist) and inhibits the transmembrane influx of calcium ions into cardiac muscle and smooth muscle. The contractile processes of cardiac muscle and vascular smooth muscle are dependent upon the movement of extracellular calcium ions into these cells through specific ion channels. Nifedipine selectively inhibits calcium ion influx across the cell membrane of cardiac muscle and vascular smooth muscle without altering serum calcium concentrations.
Mechanism of Action
A) Angina The precise mechanisms by which inhibition of calcium influx relieves angina has not been fully determined, but includes at least the following two mechanisms:
1) Relaxation and Prevention of Coronary Artery Spasm Nifedipine dilates the main coronary arteries and coronary arterioles, both in normal and ischemic regions, and is a potent inhibitor of coronary artery spasm, whether spontaneous or ergonovine-induced. This property increases myocardial oxygen delivery in patients with coronary artery spasm, and is responsible for the effectiveness of nifedipine in vasospastic (Prinzmetal’s or variant) angina. Whether this effect plays any role in classical angina is not clear, but studies of exercise tolerance have not shown an increase in the maximum exercise rate-pressure product, a widely accepted measure of oxygen utilization. This suggests that, in general, relief of spasm or dilation of coronary arteries is not an important factor in classical angina.
2) Reduction of Oxygen Utilization Nifedipine regularly reduces arterial pressure at rest and at a given level of exercise by dilating peripheral arterioles and reducing the total peripheral vascular resistance (afterload) against which the heart works. This unloading of the heart reduces myocardial energy consumption and oxygen requirements, and probably accounts for the effectiveness of nifedipine in chronic stable angina.
B) Hypertension The mechanism by which nifedipine reduces arterial blood pressure involves peripheral arterial vasodilatation and the resulting reduction in peripheral vascular resistance. The increased peripheral vascular resistance that is an underlying cause of hypertension results from an increase in active tension in the vascular smooth muscle. Studies have demonstrated that the increase in active tension reflects an increase in cytosolic free calcium.
Nifedipine is a peripheral arterial vasodilator which acts directly on vascular smooth muscle. The binding of nifedipine to voltage-dependent and possibly receptor-operated channels in vascular smooth muscle results in an inhibition of calcium influx through these channels. Stores of intracellular calcium in vascular smooth muscle are limited and thus dependent upon the influx of extracellular calcium for contraction to occur. The reduction in calcium influx by nifedipine causes arterial vasodilation and decreased peripheral vascular resistance which results in reduced arterial blood pressure.
HOW SUPPLIED
Nifedipine Extended-Release Tablets, USP are 90 mg round, biconvex, pink, film‑coated tablets imprinted with “SL503 90” on one side and plain on the other side, supplied in bottles of 100 (NDC 70807-503-12) and bottles of 300 (NDC 70807-503-13).
Store at 20˚C to 25˚C (68˚F to 77˚F), excursions permitted between 15˚C and 30˚C (59˚F and 86˚F) [see USP Controlled Room Temperature].
Protect from moisture and humidity.
Manufactured for: ELITE Pharmaceutical Solution, Inc.
Manufactured by: Patheon Pharmaceuticals Inc. 2110 E Galbraith Rd Cincinnati, Ohio 45237
Revised October 2021