Get your patient on Minocycline Hydrochloride - Minocycline Hydrochloride capsule (Minocycline Hydrochloride)
Minocycline Hydrochloride - Minocycline Hydrochloride capsule prescribing information
INDICATIONS AND USAGE
Minocycline hydrochloride capsules, USP are indicated in the treatment of the following infections due to susceptible strains of the designated microorganisms:
Rocky Mountain spotted fever, typhus fever and the typhus group, Q fever, rickettsialpox and tick fevers caused by rickettsiae.
Respiratory tract infections caused by Mycoplasma pneumoniae .
Lymphogranuloma venereum caused by Chlamydia trachomatis .
Psittacosis (Ornithosis) due to Chlamydophila psittaci.
Trachoma caused by Chlamydia trachomatis , although the infectious agent is not always eliminated, as judged by immunofluorescence.
Inclusion conjunctivitis caused by Chlamydia trachomatis .
Nongonococcal urethritis, endocervical, or rectal infections in adults caused by Ureaplasma urealyticum or Chlamydia trachomatis .
Relapsing fever due to Borrelia recurrentis .
Chancroid caused by Haemophilus ducreyi .
Plague due to Yersinia pestis .
Tularemia due to Francisella tularensis .
Cholera caused by Vibrio cholerae.
Campylobacter fetus infections caused by Campylobacter fetus.
Brucellosis due to Brucella species (in conjunction with streptomycin).
Bartonellosis due to Bartonella bacilliformis .
Granuloma inguinale caused by Klebsiella granulomatis.
Minocycline is indicated for the treatment of infections caused by the following gram-negative microorganisms when bacteriologic testing indicates appropriate susceptibility to the drug:
Escherichia coli.
Klebsiella aerogenes.
Shigella species.
Acinetobacter species.
Respiratory tract infections caused by Haemophilus influenzae .
Respiratory tract and urinary tract infections caused by Klebsiella species.
Minocycline hydrochloride capsules, USP are indicated for the treatment of infections caused by the following gram-positive microorganisms when bacteriologic testing indicates appropriate susceptibility to the drug:
Upper respiratory tract infections caused by Streptococcus pneumoniae .
Skin and skin structure infections caused by Staphylococcus aureus . (NOTE: Minocycline is not the drug of choice in the treatment of any type of staphylococcal infection.)
When penicillin is contraindicated, minocycline is an alternative drug in the treatment of the following infections:
Uncomplicated urethritis in men due to Neisseria gonorrhoeae and for the treatment of other gonococcal infections.
Infections in women caused by Neisseria gonorrhoeae .
Syphilis caused by Treponema pallidum subspecies pallidum .
Yaws caused by Treponema pallidum subspecies pertenue .
Listeriosis due to Listeria monocytogenes .
Anthrax due to Bacillus anthracis.
Vincent’s infection caused by Fusobacterium fusiforme .
Actinomycosis caused by Actinomyces israelii .
Infections caused by Clostridium species.
In acute intestinal amebiasis, minocycline may be a useful adjunct to amebicides.
In severe acne , minocycline may be useful adjunctive therapy.
Oral minocycline is indicated in the treatment of asymptomatic carriers of Neisseria meningitidis to eliminate meningococci from the nasopharynx. In order to preserve the usefulness of minocycline in the treatment of asymptomatic meningococcal carriers, diagnostic laboratory procedures, including serotyping and susceptibility testing, should be performed to establish the carrier state and the correct treatment. It is recommended that the prophylactic use of minocycline be reserved for situations in which the risk of meningococcal meningitis is high.
Oral minocycline is not indicated for the treatment of meningococcal infection.
Although no controlled clinical efficacy studies have been conducted, limited clinical data show that oral minocycline hydrochloride has been used successfully in the treatment of infections caused by Mycobacterium marinum .
To reduce the development of drug-resistant bacteria and maintain the effectiveness of minocycline hydrochloride capsules, USP and other antibacterial drugs, minocycline hydrochloride capsules, USP should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
DOSAGE & ADMINISTRATION
THE USUAL DOSAGE AND FREQUENCY OF ADMINISTRATION OF MINOCY‑CLINE DIFFERS FROM THAT OF THE OTHER TETRACYCLINES. EXCEEDING THE RECOMMENDED DOSAGE MAY RESULT IN AN INCREASED INCIDENCE OF SIDE EFFECTS.
Minocycline hydrochloride capsules USP may be taken with or without food (see CLINICAL PHARMACOLOGY ).
Ingestion of adequate amounts of fluids along with capsule and tablet forms of drugs in the tetracycline-class is recommended to reduce the risk of esophageal irritation and ulceration. The capsules should be swallowed whole.
For Pediatric Patients above 8 Years of Age
Usual pediatric dose: 4 mg/kg initially followed by 2 mg/kg every 12 hours, not to exceed the usual adult dose.
Adults
The usual dosage of minocycline hydrochloride capsules USP is 200 mg initially followed by 100 mg every 12 hours. Alternatively, if more frequent doses are preferred, two or four 50 mg capsules may be given initially followed by one 50 mg capsule 4 times daily.
Uncomplicated gonococcal infections other than urethritis and anorectal infec‑tions in men: 200 mg initially, followed by 100 mg every 12 hours for a minimum of 4 days, with post-therapy cultures within 2 to 3 days.
In the treatment of uncomplicated gonococcal urethritis in men, 100 mg every 12 hours for 5 days is recommended.
For the treatment of syphilis, the usual dosage of minocycline hydrochloride should be administered over a period of 10 to 15 days. Close follow-up, including laboratory tests, is recommended.
In the treatment of meningococcal carrier state, the recommended dosage is 100 mg every 12 hours for 5 days.
Mycobacterium marinum infections: Although optimal doses have not been established, 100 mg every 12 hours for 6 to 8 weeks have been used successfully in a limited number of cases.
Uncomplicated urethral, endocervical, or rectal infection in adults caused by Chlamydia trachomatis or Ureaplasma urealyticum : 100 mg orally, every 12 hours for at least 7 days.
Ingestion of adequate amounts of fluids along with capsule and tablet forms of drugs in the tetracycline-class is recommended to reduce the risk of esophageal irritation and ulceration.
The pharmacokinetics of minocycline in patients with renal impairment (CL CR <80 mL/min) have not been fully characterized. Current data are insufficient to determine if a dosage adjustment is warranted. The total daily dosage should not exceed 200 mg in 24 hours. However, due to the antianabolic effect of tetracyclines, BUN and creatinine should be monitored (See WARNINGS-Antianabolic Action ).
CONTRAINDICATIONS
This drug is contraindicated in persons who have shown hypersensitivity to any of the tetracyclines or to any of the components of the product formulation.
ADVERSE REACTIONS
Due to oral minocycline’s virtually complete absorption, side effects to the lower bowel, particularly diarrhea, have been infrequent. The following adverse reactions have been observed in patients receiving tetracyclines:
Body as a whole: Fever, and discoloration of secretions.
Gastrointestinal: Anorexia, nausea, vomiting, diarrhea, dyspepsia, stomatitis, glossitis, dysphagia, enamel hypoplasia, enterocolitis, pseudomembranous colitis, pancreatitis, inflammatory lesions (with monilial overgrowth) in the oral and anogenital regions. Instances of esophagitis and esophageal ulcerations have been reported in patients taking the tetracycline-class antibiotics in capsule and tablet form. Most of these patients took the medication immediately before going to bed (see DOSAGE AND ADMINISTRATION ).
Genitourinary: Vulvovaginitis.
Hepatic toxicity: Hyperbilirubinemia, hepatic cholestasis, increases in liver enzymes, fatal hepatic failure, and jaundice. Hepatitis, including autoimmune hepatitis, and liver failure have been reported (see PRECAUTIONS ).
Skin: Alopecia, erythema nodosum, hyperpigmentation of nails, pruritus, toxic epidermal necrolysis, vasculitis, maculopapular rash and erythematous rash. Exfoliative dermatitis has been reported. Fixed drug eruptions have been report‑ed. Lesions occurring on the glans penis have caused balanitis. Erythema multiforme and Stevens-Johnson syndrome have been reported. Photosensitivity is discussed above (see WARNINGS-Photosensitivity ). Pigmentation of the skin and mucous membranes has been reported.
Respiratory: Cough, dyspnea, bronchospasm, exacerbation of asthma, and pneumonitis.
Renal toxicity: Interstitial nephritis. Elevations in BUN have been reported and are apparently dose related (see WARNINGS ). Reversible acute renal failure has been reported.
Musculoskeletal: Arthralgia, arthritis, bone discoloration, myalgia, joint stiff‑ness, and joint swelling.
Hypersensitivity reactions: Urticaria, angioneurotic edema, polyarthralgia, anaphylaxis/anaphylactoid reaction (including shock and fatalities), anaphylactoid purpura, myocarditis, pericarditis, exacerbation of systemic lupus erythematosus and pulmonary infiltrates with eosinophilia have been reported. A transient lupus-like syndrome and serum sickness-like reactions also have been reported.
Blood: Agranulocytosis, hemolytic anemia, thrombocytopenia, leukopenia, neutropenia, pancytopenia, and eosinophilia have been reported.
Central Nervous System: Convulsions, dizziness, hypesthesia, paresthesia, sedation, and vertigo. Bulging fontanels in infants and benign intracranial hypertension (pseudotumor cerebri) in adults have been reported (see WARNINGS-Intracranial Hypertension ). Headache has also been reported.
Other: Thyroid cancer has been reported in the post-marketing setting in association with minocycline products. When minocycline therapy is given over prolonged periods, monitoring for signs of thyroid cancer should be considered. When given over prolonged periods, tetracyclines have been reported to produce brown-black microscopic discoloration of the thyroid gland. Cases of abnormal thyroid function have been reported.
Tooth discoloration in children less than 8 years of age (see WARNINGS-Tooth Development ) and also, in adults has been reported.
Oral cavity discoloration (including tongue, lip, and gum) has been reported. Tinnitus and decreased hearing have been reported in patients on minocycline hydrochloride capsules.
The following syndromes have been reported. In some cases involving these syndromes, death has been reported. As with other serious adverse reactions, if any of these syndromes are recognized, the drug should be discontinued immediately:
Hypersensitivity syndrome consisting of cutaneous reaction (such as rash or exfoliative dermatitis), eosinophilia, and one or more of the following: hepatitis, pneumonitis, nephritis, myocarditis, and pericarditis. Fever and lymphadenopathy may be present.
Lupus-like syndrome consisting of positive antinuclear antibody; arthralgia, arthritis, joint stiffness, or joint swelling; and one or more of the following: fever, myalgia, hepatitis, rash, and vasculitis.
Serum sickness-like syndrome consisting of fever; urticaria or rash; and arthralgia, arthritis, joint stiffness, or joint swelling and lymphadenopathy.
Eosinophilia may be present.
Post-Marketing Experience
The following adverse reaction has been identified during post-approval use of minocycline products when taken orally. Because this reaction is reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Skin and hypersensitivity reactions: Acute febrile neutrophilic dermatosis (Sweet’s syndrome).
To report SUSPECTED ADVERSE REACTIONS, contact Sun Pharmaceutical Industries, Inc. at 1-800-818-4555 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Because tetracyclines have been shown to depress plasma prothrombin activity, patients who are on anticoagulant therapy may require downward adjustment of their anticoagulant dosage.
Since bacteriostatic drugs may interfere with the bactericidal action of penicillin, it is advisable to avoid giving tetracycline-class drugs in conjunction with penicillin.
Absorption of tetracyclines is impaired by antacids containing aluminum, calcium, or magnesium, and iron-containing preparations.
Concurrent use of tetracyclines with oral contraceptives may render oral contraceptives less effective.
Administration of isotretinoin should be avoided shortly before, during, and shortly after minocycline therapy. Each drug alone has been associated with pseudotumor cerebri (See WARNINGS ).
Increased risk of ergotism when ergot alkaloids or their derivatives are given with tetracyclines.
DESCRIPTION
Minocycline hydrochloride USP, is a semisynthetic derivative of tetracycline, 4,7-Bis(dimethylamino)-1,4,4a,5,5a,6,11,12a-octahydro-3,10,12,12a-tetrahydroxy-1,11-dioxo-2-naphthacenecarboxamide monohydrochloride.
Its structural formula is:
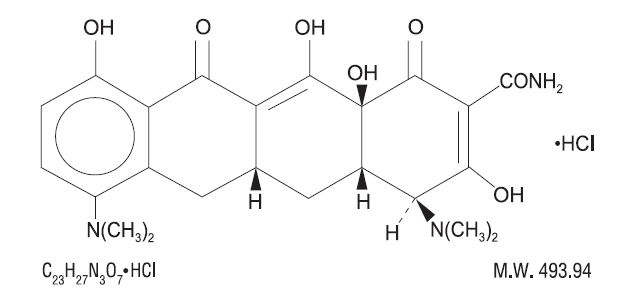 C 23 H 27 N 3 O 7 •HCl M.W. 493.94
C 23 H 27 N 3 O 7 •HCl M.W. 493.94
Minocycline hydrochloride capsules USP for oral administration contain minocycline hydrochloride, USP equivalent to 50 mg, 75 mg, or 100 mg of minocycline and the following inactive ingredients: lactose monohydrate, microcrystalline cellulose, povidone, sodium starch glycolate, colloidal silicon dioxide, magnesium stearate, titanium dioxide, gelatin, D&C Yellow #10 aluminum lake, FD&C Blue #1 aluminum lake, FD&C Blue #2 aluminum lake, FD&C Red #40 aluminum lake, black iron oxide, propylene glycol and shellac.
In addition 50 mg capsules contains D&C Red #33 aluminum lake, FD&C Red #3 aluminum lake and FD&C Yellow #6 aluminum lake; 75 mg capsules contains FDA/E172 black iron oxide and 100 mg capsules contains D&C Red #28 aluminum lake, FD&C Blue #1 aluminum lake, FD&C Red #40 aluminum lake and FDA/E172 red iron oxide.
CLINICAL PHARMACOLOGY
Following a single dose of two 100 mg capsules of minocycline hydrochloride administered to 18 normal fasting adult volunteers, maximum serum concentrations were attained in 1 to 4 hours (average 2.1 hours) and ranged from 2.1 to 5.1 mcg/mL (average 3.5 mcg/mL). The serum half-life in the normal volunteers ranged from 11.1 to 22.1 hours (average 15.5 hours).
When minocycline hydrochloride capsules were given concomitantly with a high-fat meal, which included dairy products, the extent of absorption of minocycline hydrochloride capsules was unchanged compared to dosing under fasting conditions. The mean T max was delayed by 1 hour when administered with food, compared to dosing under fasting conditions.
Minocycline capsules may be administered with or without food.
In previous studies with other minocycline dosage forms, the minocycline serum half-life ranged from 11 to 16 hours in 7 patients with hepatic dysfunction, and from 18 to 69 hours in 5 patients with renal dysfunction. The urinary and fecal recovery of minocycline when administered to 12 normal volunteers was one-half to one-third that of other tetracyclines.
Microbiology
Mechanism of Action
The tetracyclines are primarily bacteriostatic and are thought to exert their antimicrobial effect by the inhibition of protein synthesis. The tetracyclines, including minocycline, have a similar antimicrobial spectrum of activity against a wide range of gram-positive and gram-negative organisms. Cross-resistance of these organisms to tetracycline is common.
Antimicrobial Activity
Minocycline has been shown to be active against most strains of the following microorganisms, both in vitro and in clinical infections (see INDICATIONS AND USAGE ).
Gram-positive Bacteria
Bacillus anthracis
Listeria monocytogenes
Staphylococcus aureus
Streptococcus pneumoniae
Gram-negative Bacteria
Acinetobacter species
Bartonella bacilliformis
Brucella species
Campylobacter fetus
Escherichia coli
Francisella tularensis
Haemophilus ducreyi
Haemophilus influenzae
Klebsiella aerogenes
Klebsiella granulomatis
Klebsiella species
Neisseria gonorrhoeae
Neisseria meningitidis
Shigella species
Yersinia pestis
Vibrio cholerae
Other Microorganisms
Actinomyces species
Borrelia recurrentis
Chlamydophila psittaci
Chlamydia trachomatis
Clostridium species
Entamoeba species
Fusobacterium nucleatum subspecies fusiforme
Mycobacterium marinum
Mycoplasma pneumoniae
Propionibacterium acnes
Rickettsiae
Treponema pallidum subspecies pallidum
Treponema pallidum subspecies pertenue
Ureaplasma urealyticum .
Susceptibility Testing
For specific information regarding susceptibility test interpretive criteria and associated test methods and quality control standards recognized by the FDA for this drug, please see https://www.fda.gov/STIC.
HOW SUPPLIED
Minocycline hydrochloride Capsules USP, 50 mg are Flesh Opaque/ Flesh Opaque colored hard gelatin capsules, imprinted with ‘851’ on both cap and body in black ink available as follows:
Bottles of 100 NDC 57664-851-88
Bottles of 500 NDC 57664-851-13
Minocycline hydrochloride Capsules USP, 75 mg are Gray Opaque/Gray Opaque colored hard gelatin capsules, imprinted with ‘852’ on both cap and body in black ink available as follows:
Bottles of 100 NDC 57664-852-88
Bottles of 500 NDC 57664-852-13
Minocycline hydrochloride Capsules USP, 100 mg are Maroon Opaque/ Flesh Opaque colored hard gelatin capsules, imprinted with ‘853’ on both cap and body in black ink available as follows:
Bottles of 50 NDC 57664-853-85
Bottles of 500 NDC 57664-853-13
Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required).
Protect from light, moisture and excessive heat.
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].