Get your patient on Metopirone (Metyrapone)
Metopirone prescribing information
INDICATIONS AND USAGE
Metopirone is indicated, in combination with other diagnostic tests, for the diagnosis of adrenal insufficiency in adult and pediatric patients.
DOSAGE AND ADMINISTRATION
- Single-Dose Short Test: 30 mg/kg at midnight (2.2 )
Important Information Before Conducting Metopirone Testing
Stop drugs affecting pituitary or adrenocortical function before administration of Metopirone in accordance with half-life of the drugs (consider at least 5 half-lives to avoid any interference with Metopirone testing). [see Drug Interactions (7.1) ] .
Assess ability of patient's adrenals to respond to exogenous ACTH before Metopirone is employed as a test [see Warnings and Precautions (5.1) ] .
Single-Dose Short Test- Recommended Dose and Interpretation
This test, usually given on an outpatient basis, determines plasma 11-desoxycortisol and/or ACTH levels after a single dose of Metopirone. Patients with suspected adrenocortical insufficiency based on the test results previously performed should be hospitalized overnight as a precautionary measure ( see Warnings and Precaution (5.1) ).
Recommended Dose
In adult and pediatric patients, the recommended single dose is 30 mg/kg (maximum 3 grams of Metopirone) administered at midnight with milk/yogurt or snack. The blood sample for the assay is taken early the following morning (7:30-8:00 a.m.). After the blood sample is collected, a prophylactic dose of glucocorticoid may be considered for patients with high risk for acute adrenal insufficiency.
Interpretation of 11‑desoxycortisol and ACTH Levels After Metopirone Administration
Approximately 8 hours after administration of Metopirone, evaluate the values of ACTH and 11-desoxycortisol. Normal values will depend on the method used to determine ACTH and 11‑desoxycortisol levels. An intact HPA axis function is generally indicated by an increase in 11‑desoxycortisol to over 70 mcg/L. Because of an overlap between a normal ACTH response and an abnormal ACTH response, the ACTH response alone cannot be used to distinguish between healthy individuals and those with adrenal insufficiency.
DOSAGE FORMS AND STRENGTHS
Capsules: Metopirone 250 mg soft gelatin, white to yellowish‑white, oblong, opaque, imprinted with "HRA" on one side in red ink.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
Available data from published case series and reports on Metopirone use in pregnant females are insufficient to identify a drug-associated risk of major birth defects or miscarriage. Metyrapone crosses the placenta and may decrease fetal cortisol production (see Data ) . Animal reproductive studies have not been conducted with metyrapone. Metyrapone can decrease reproductive hormones by targeting adrenal androgenesis.
Data
Human Data
The Metopirone test was administered to pregnant women in their second and third trimester of pregnancy and evidence was found that the fetal pituitary responded to the enzymatic block. Transplacental transfer of Metopirone has been shown in humans and the drug can impair the biosynthesis of fetal and placental steroids. There are a few published reports of low cortisol levels at birth in infants exposed in utero following chronic use of metyrapone in pregnant females.
Lactation
Risk Summary
Metyrapone and its active metabolite, metyrapol, are present in human milk. There are no available data on the effects of metyrapone on the breastfed infant or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for Metopirone and any potential adverse effects on the breastfed infant from Metopirone or from the underlying maternal condition.
Pediatric Use
Metopirone is indicated, in combination with other diagnostic tests, for the diagnosis of adrenal insufficiency in pediatric patients [See Dosage and Administration (2.1) ].
Geriatric Use
Clinical studies of Metopirone did not include sufficient numbers of patients 65 years of age and older to determine whether they respond differently from younger adult patients.
Other reported clinical experience has not identified differences in responses between patients 65 years of age and older and younger adult patients.
Hepatic Impairment
Patients with cirrhosis may have an impaired response to Metopirone.
CONTRAINDICATIONS
Metopirone is contraindicated in patients with adrenal cortical insufficiency or hypersensitivity to Metopirone or to any of its excipients.
WARNINGS AND PRECAUTIONS
- Adrenal Insufficiency: May induce acute adrenal insufficiency. Ability of adrenals to respond to exogenous ACTH should be demonstrated before Metopirone is employed as a test (5.1 )
- Dizziness and Sedation: May cause dizziness and sedation. Patients should not drive or operate machinery until these effects have passed (5.2 )
Adrenal Insufficiency
Metopirone may induce acute adrenal insufficiency in patients with reduced adrenal secretory capacity, as well as in patients with global pituitary insufficiency. The test should be performed in the hospital with close monitoring in case of suspected adrenal insufficiency.
Ability of adrenals to respond to exogenous ACTH should be demonstrated before Metopirone is employed as a test.
In the presence of hypo‑ or hyperthyroidism, response to the Metopirone test may be subnormal.
If adrenocortical or anterior pituitary function is more severely compromised than indicated by the results of the test, Metopirone may trigger adrenal insufficiency. This can be corrected by giving appropriate doses of corticosteroids.
Dizziness and Sedation
Metopirone may cause dizziness and sedation. Patients should not drive or operate machinery until these effects have passed.
ADVERSE REACTIONS
The following adverse reactions associated with the use of Metopirone were identified in clinical trials or postmarketing reports. Because these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Cardiovascular System: Hypotension
- Gastrointestinal System: Nausea, vomiting, abdominal discomfort or pain
- Central Nervous System: Headache, dizziness, sedation
- Dermatologic System: Allergic rash
- Hematologic System: Leukopenia, anemia, and/or thrombocytopenia
DRUG INTERACTIONS
Effect of Other Drugs on Metopirone
Anticonvulsants, psychotropic drugs, hormone preparations, corticosteroids, antithyroid agents and cyproheptadine may affect the results of the Metopirone test.
If these drugs cannot be withdrawn, the necessity of carrying out the Metopirone test should be reviewed.
Effect of Metopirone on Other Drugs
Acetaminophen
Metopirone inhibits the glucuronidation of acetaminophen, which may decrease elimination of acetaminophen and lead to increased risk of adverse reactions related to acetaminophen.
Avoid concomitant use of Metopirone with acetaminophen.
DESCRIPTION
Metopirone (metyrapone capsules) is an adrenal steroid synthesis inhibitor, available as 250‑mg capsules for oral administration. Its chemical name is 2‑methyl‑1, 2‑di‑3‑pyridyl‑1‑propanone, and its structural formula is
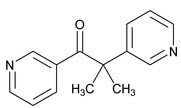
Metyrapone is a white to light amber, fine, crystalline powder, having a characteristic odor. It is sparingly soluble in water, and soluble in methanol and in chloroform. It forms water‑soluble salts with acids. Its molecular weight is 226.27.
Inactive Ingredients : Ethyl vanillin, gelatin, glycerol, macrogol 400, macrogol 4000, paramethoxy acetophenone, purified water, sodium ethyl parahydroxybenzoate, sodium propyl parahydroxybenzoate, titanium dioxide, + red ink (aluminum chloride hexahydrate, carminic acid, hypromellose, propylene glycol, sodium hydroxide).
CLINICAL PHARMACOLOGY
Mechanism of Action
The pharmacological effect of Metopirone is to reduce cortisol and corticosterone production by inhibiting the 11-beta-hydroxylation reaction in the adrenal cortex. Removal of the strong inhibitory feedback mechanism exerted by cortisol results in an increase in adrenocorticotropic hormone (ACTH) production by the pituitary. With continued blockade of the enzymatic steps leading to production of cortisol and corticosterone, there is a marked increase in adrenocortical secretion of their immediate precursors, 11-desoxycortisol and desoxycorticosterone, which are weak suppressors of ACTH release, and a corresponding elevation of these steroids in the plasma and of their metabolites in the urine. These metabolites are readily determined by measuring urinary 17‑hydroxycorticosteroids (17-OHCS) or 17-ketogenic steroids (17-KGS). Because of these actions, Metopirone is used as a diagnostic test, with urinary 17-OHCS measured as an index of pituitary ACTH responsiveness. Metopirone may also suppress biosynthesis of aldosterone, resulting in a mild natriuresis.
Pharmacodynamics
Metopirone exposure-response relationships and the time course of pharmacodynamic response are unknown.
Pharmacokinetics
The mean C max of metyrapone following a single 750 mg is 3.7 mcg/mL falling to 0.5 mcg/mL 4 hours after administration.
Absorption
The time to peak plasma concentration of metyrapone is approximately 1 hour after oral administration.
Elimination
The mean (± SD) terminal elimination half‑lives of metyrapone and its active metabolite metyrapol are 1.9 (± 0.7) hours and approximately 4 hours, respectively.
Metabolism
Metyrapone is reduced to metyrapol, an active alcohol metabolite. Both metyrapone and metyrapol are conjugated with glucuronide.
Eight hours after a single oral dose, the ratio of metyrapone to its active metabolite metyrapol in plasma is 1:1.5.
Excretion
Following administration of metyrapone 750 mg every 4 hours, approximately 5.3% of the dose was excreted in urine as unchanged and 38.5% as its active metabolite metyrapol within 72 hours after the first dose.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Long‑term animal carcinogenicity studies have not been conducted with Metopirone.
Mutagenesis
Metyrapone was not mutagenic with or without metabolic activation in bacterial mutagenicity tests.
Impairment of Fertility
No studies have been conducted to assess the effect of Metopirone on fertility.
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
Metopirone (metyrapone capsules) are supplied as 250 mg soft gelatin, white to yellowish‑white, oblong, opaque capsules, imprinted with "HRA" on one side in red ink.
Bottle of 18 capsules: NDC 76336-455-18
Storage and Handling
Store Metopirone bottles at room temperature 20°C to 25°C (68°F to 77°F), excursions permitted between 15°C and 30°C (59°F and 86°F) [see USP Controlled Room Temperature].
Keep container tightly closed and protect from heat and moisture.
Mechanism of Action
The pharmacological effect of Metopirone is to reduce cortisol and corticosterone production by inhibiting the 11-beta-hydroxylation reaction in the adrenal cortex. Removal of the strong inhibitory feedback mechanism exerted by cortisol results in an increase in adrenocorticotropic hormone (ACTH) production by the pituitary. With continued blockade of the enzymatic steps leading to production of cortisol and corticosterone, there is a marked increase in adrenocortical secretion of their immediate precursors, 11-desoxycortisol and desoxycorticosterone, which are weak suppressors of ACTH release, and a corresponding elevation of these steroids in the plasma and of their metabolites in the urine. These metabolites are readily determined by measuring urinary 17‑hydroxycorticosteroids (17-OHCS) or 17-ketogenic steroids (17-KGS). Because of these actions, Metopirone is used as a diagnostic test, with urinary 17-OHCS measured as an index of pituitary ACTH responsiveness. Metopirone may also suppress biosynthesis of aldosterone, resulting in a mild natriuresis.