Furosemide - Furosemide tablet prescribing information
INDICATIONS AND USAGE
Edema
Furosemide tablets are indicated in adults and pediatric patients for the treatment of edema associated with congestive heart failure, cirrhosis of the liver, and renal disease, including the nephrotic syndrome. Furosemide is particularly useful when an agent with greater diuretic potential is desired.
Hypertension
Oral furosemide may be used in adults for the treatment of hypertension alone or in combination with other antihypertensive agents. Hypertensive patients who cannot be adequately controlled with thiazides will probably also not be adequately controlled with furosemide alone.
DOSAGE AND ADMINISTRATION
Edema
Therapy should be individualized according to patient response to gain maximal therapeutic response and to determine the minimal dose needed to maintain that response.
Adults
The usual initial dose of oral furosemide is 20 to 80 mg given as a single dose. Ordinarily a prompt diuresis ensues. If needed, the same dose can be administered 6 to 8 hours later or the dose may be increased. The dose may be raised by 20 or 40 mg and given not sooner than 6 to 8 hours after the previous dose until the desired diuretic effect has been obtained. The individually determined single dose should then be given once or twice daily (e.g., at 8 a.m. and 2 p.m.). The dose of furosemide may be carefully titrated up to 600 mg/day in patients with clinically severe edematous states.
Edema may be most efficiently and safely mobilized by giving furosemide on 2 to 4 consecutive days each week.
When doses exceeding 80 mg/day are given for prolonged periods, careful clinical observation and laboratory monitoring are particularly advisable (see PRECAUTIONS, Laboratory Tests ).
Geriatric Patients
In general, dose selection for the elderly patient should be cautious, usually starting at the low end of the dosing range (see PRECAUTIONS, Geriatric Use ).
Pediatric Patients
The usual initial dose of oral furosemide in pediatric patients is 2 mg/kg body weight given as a single dose. If the diuretic response is not satisfactory after the initial dose, dosage may be increased by 1 or 2 mg/kg no sooner than 6 to 8 hours after the previous dose. Doses greater than 6 mg/kg body weight are not recommended. For maintenance therapy in pediatric patients, the dose should be adjusted to the minimum effective level.
Hypertension
Therapy should be individualized according to the patient’s response to gain maximal therapeutic response and to determine the minimal dose needed to maintain that therapeutic response.
Adults
The usual initial dose of furosemide for hypertension is 80 mg, usually divided into 40 mg twice a day. Dosage should then be adjusted according to response. If response is not satisfactory, add other antihypertensive agents.
Changes in blood pressure must be carefully monitored when furosemide is used with other antihypertensive drugs, especially during initial therapy. To prevent excessive drop in blood pressure, the dosage of other agents should be reduced by at least 50 percent when furosemide is added to the regimen. As the blood pressure falls under the potentiating effect of furosemide, a further reduction in dosage or even discontinuation of other antihypertensive drugs may be necessary.
Geriatric Patients
In general, dose selection and dose adjustment for the elderly patient should be cautious, usually starting at the low end of the dosing range (see PRECAUTIONS, Geriatric Use ).
CONTRAINDICATIONS
Furosemide is contraindicated in patients with anuria and in patients with a history of hypersensitivity to furosemide.
ADVERSE REACTIONS
Adverse reactions are categorized below by organ system and listed by decreasing severity.
Gastrointestinal System Reactions
- hepatic encephalopathy in patients with hepato-cellular insufficiency
- pancreatitis
- jaundice (intrahepatic cholestatic jaundice)
- increased liver enzymes
- anorexia
- oral and gastric irritation
- cramping
- diarrhea
- constipation
- nausea
- vomiting
Systemic Hypersensitivity Reactions
- Severe anaphylactic or anaphylactoid reactions (e.g. with shock)
- systemic vasculitis
- interstitial nephritis
- necrotizing angiitis
Central Nervous System Reactions
- tinnitus and hearing loss
- paresthesias
- vertigo
- dizziness
- headache
- blurred vision
- xanthopsia
Hematologic Reactions
- aplastic anemia
- thrombocytopenia
- agranulocytosis
- hemolytic anemia
- leukopenia
- anemia
- eosinophilia
Dermatologic-Hypersensitivity Reactions
- toxic epidermal necrolysis
- Stevens-Johnson Syndrome
- erythema multiforme
- drug rash with eosinophilia and systemic symptoms
- acute generalized exanthematous pustulosis
- exfoliative dermatitis
- bullous pemphigoid
- purpura
- photosensitivity
- rash
- pruritis
- urticaria
Cardiovascular Reaction
- Orthostatic hypotension may occur and be aggravated by alcohol, barbiturates or narcotics.
- Increase in cholesterol and triglyceride serum levels
Other Reactions
- hyperglycemia
- glycosuria
- hyperuricemia
- muscle spasm
- weakness
- restlessness
- urinary bladder spasm
- thrombophlebitis
- fever
Whenever adverse reactions are moderate or severe, furosemide dosage should be reduced or therapy withdrawn.
DESCRIPTION
Furosemide, USP is a diuretic which is an anthranilic acid derivative. Chemically, it is 4-chloro-N-furfuryl-5-sulfamoylanthranilic acid. Furosemide, USP is a white to slightly yellow, odorless, crystalline powder. It is practically insoluble in water, sparingly soluble in alcohol, freely soluble in solutions of dilute alkali hydroxides and insoluble in dilute acids.
The CAS Registry Number is 54-31-9.
The structural formula is as follows:
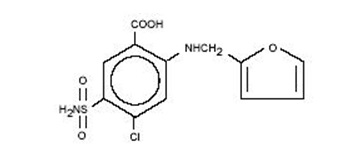
C 12 H 11 ClN 2 O 5 S M.W. 330.74
Each tablet, for oral administration, contains 20 mg or 40 mg Furosemide, USP. In addition, each tablet contains the following inactive ingredients: colloidal silicon dioxide, corn starch, lactose monohydrate, magnesium stearate, povidone, and sodium starch glycolate.
Both strengths: 20 mg and 40 mg meet USP Dissolution Test 1.
CLINICAL PHARMACOLOGY
Investigations into the mode of action of furosemide have utilized micropuncture studies in rats, stop flow experiments in dogs, and various clearance studies in both humans and experimental animals. It has been demonstrated that furosemide inhibits primarily the absorption of sodium and chloride not only in the proximal and distal tubules but also in the loop of Henle. The high degree of efficacy is largely due to the unique site of action. The action on the distal tubule is independent of any inhibitory effect on carbonic anhydrase and aldosterone.
Recent evidence suggests that furosemide glucuronide is the only or at least the major biotransformation product of furosemide in man. Furosemide is extensively bound to plasma proteins, mainly to albumin. Plasma concentrations ranging from 1 to 400 mcg/mL are 91 to 99% bound in healthy individuals. The unbound fraction averages 2.3 to 4.1% at therapeutic concentrations.
The onset of diuresis following oral administration is within 1 hour. The peak effect occurs within the first or second hour. The duration of diuretic effect is 6 to 8 hours.
In fasted normal men, the mean bioavailability of furosemide from furosemide tablets and furosemide oral solution is 64% and 60%, respectively, of that from an intravenous injection of the drug. Although furosemide is more rapidly absorbed from the oral solution (50 minutes) than from the tablet (87 minutes), peak plasma levels and area under the plasma concentration-time curves do not differ significantly. Peak plasma concentrations increase with increasing dose but times-to-peak do not differ among doses. The terminal half-life of furosemide is approximately 2 hours.
Significantly more furosemide is excreted in urine following the IV injection than after the tablet or oral solution. There are no significant differences between the two oral formulations in the amount of unchanged drug excreted in urine.
Geriatric Population
Furosemide binding to albumin may be reduced in elderly patients. Furosemide is predominantly excreted unchanged in the urine. The renal clearance of furosemide after intravenous administration in older healthy male subjects (60 to 70 years of age) is statistically significantly smaller than in younger healthy male subjects (20 to 35 years of age). The initial diuretic effect of furosemide in older subjects is decreased relative to younger subjects (see PRECAUTIONS, Geriatric Use ).
HOW SUPPLIED
Furosemide Tablets, USP 20 mg are available as white, round, flat face, beveled edge, tablets debossed “ CE ” on one side and “ 174 ” on the other side, containing 20 mg of Furosemide, USP and supplied as follows:
NDC 62135-753-90 in bottles of 90 tablets
Furosemide Tablets, USP 40 mg are available as white, round, flat face, beveled edge bisected debossed with “ CE ” on one side of the break line and " 175 " on the other side containing 40 mg of Furosemide, USP and supplied as follows:
NDC 62135-754-90 in bottles of 90 tablets
Dispense in a well-closed, light-resistant container as defined in the USP, with a child-resistant closure (as required). Exposure to light may cause slight discoloration. Discolored tablets should not be dispensed.
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
KEEP THIS AND ALL MEDICATIONS OUT OF THE REACH OF CHILDREN.
Manufactured For: Chartwell RX, LLC Congers, NY 10920
Rev. 04/2024
L72083