Get your patient on Fosinopril Sodium - Fosinopirl Sodium tablet (Fosinopirl Sodium)
Fosinopril Sodium - Fosinopirl Sodium tablet prescribing information
WARNING: FETAL TOXICITY
- When pregnancy is detected, discontinue fosinopril sodium tablets as soon as possible.
- Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. See WARNINGS, Fetal TOXICITY
INDICATIONS AND USAGE
Fosinopril sodium tablets are indicated for the treatment of hypertension. They may be used alone or in combination with thiazide diuretics.
Fosinopril sodium tablets are indicated in the management of heart failure as adjunctive therapy when added to conventional therapy including diuretics with or without digitalis (see DOSAGE AND ADMINISTRATION ).
In using fosinopril sodium, consideration should be given to the fact that another angiotensin-converting enzyme inhibitor, captopril, has caused agranulocytosis, particularly in patients with renal impairment or collagen-vascular disease. Available data are insufficient to show that fosinopril sodium does not have a similar risk (see WARNINGS ).
In considering use of fosinopril sodium, it should be noted that in controlled trials ACE inhibitors have an effect on blood pressure that is less in black patients than in non-blacks. In addition, ACE inhibitors (for which adequate data are available) cause a higher rate of angioedema in black than in non-black patients (see WARNINGS , Head and Neck Angioedema and Intestinal Angioedema ).
DOSAGE AND ADMINISTRATION
Hypertension
Adults
The recommended initial dose of fosinopril sodium tablets USP is 10 mg once a day, both as monotherapy and when the drug is added to a diuretic. Dosage should then be adjusted according to blood pressure response at peak (2 to 6 hours) and trough (about 24 hours after dosing) blood levels. The usual dosage range needed to maintain a response at trough is 20 to 40 mg but some patients appear to have a further response to 80 mg. In some patients treated with once daily dosing, the antihypertensive effect may diminish toward the end of the dosing interval. If trough response is inadequate, dividing the daily dose should be considered. If blood pressure is not adequately controlled with fosinopril sodium tablets USP alone, a diuretic may be added.
Concomitant administration of fosinopril sodium tablets USP with potassium supplements, potassium salt substitutes, or potassium-sparing diuretics can lead to increases of serum potassium (see PRECAUTIONS ).
In patients who are currently being treated with a diuretic, symptomatic hypotension occasionally can occur following the initial dose of fosinopril sodium tablets USP. To reduce the likelihood of hypotension, the diuretic should, if possible, be discontinued 2 to 3 days prior to beginning therapy with fosinopril sodium tablets USP (see WARNINGS ). Then, if blood pressure is not controlled with fosinopril sodium tablets USP alone, diuretic therapy should be resumed. If diuretic therapy cannot be discontinued, an initial dose of 10 mg of fosinopril sodium tablets USP should be used with careful medical supervision for several hours and until blood pressure has stabilized (see WARNINGS and PRECAUTIONS , Information for Patients and Drug Interactions ).
Since concomitant administration of fosinopril sodium tablets USP with potassium supplements, or potassium-containing salt substitutes or potassium-sparing diuretics may lead to increases in serum potassium, they should be used with caution (see PRECAUTIONS ).
Pediatrics
In children, doses of fosinopril sodium tablets between 0.1 and 0.6 mg/kg have been studied and shown to reduce blood pressure to a similar extent (see CLINICAL PHARMACOLOGY , Pharmacodynamics and Clinical Effects ). Based on this, the recommended dose of fosinopril sodium tablets USP in children weighing more than 50 kg is 5 to 10 mg once per day as monotherapy. An appropriate dosage strength is not available for children weighing less than 50 kg.
Heart Failure
Digitalis is not required for fosinopril sodium tablets USP to manifest improvements in exercise tolerance and symptoms. Most placebo-controlled clinical trial experience has been with both digitalis and diuretics present as background therapy.
The usual starting dose of fosinopril sodium tablets USP should be 10 mg once daily. Following the initial dose of fosinopril sodium tablets USP, the patient should be observed under medical supervision for at least 2 hours for the presence of hypotension or orthostasis, and if present, until blood pressure stabilizes. An initial dose of 5 mg is preferred in heart failure patients with moderate to severe renal failure or those who have been vigorously diuresed.
Dosage should be increased, over a several week period, to a dose that is maximal and tolerated but not exceeding 40 mg once daily. The usual effective dosage range is 20 to 40 mg once daily.
The appearance of hypotension, orthostasis, or azotemia early in dose titration should not preclude further careful dose titration. Consideration should be given to reducing the dose of concomitant diuretic.
For Hypertensive or Heart Failure Patients With Renal Impairment
In patients with impaired renal function, the total body clearance of fosinoprilat is approximately 50% slower than in patients with normal renal function. Since hepatobiliary elimination partially compensates for diminished renal elimination, the total body clearance of fosinoprilat does not differ appreciably with any degree of renal insufficiency (creatinine clearances < 80 mL/min/1.73 m 2 ), including end-stage renal failure (creatinine clearance < 10 mL/min/1.73 m 2 ). This relative constancy of body clearance of active fosinoprilat, resulting from the dual route of elimination, permits use of the usual dose in patients with any degree of renal impairment (see WARNINGS , Anaphylactoid Reactions During Membrane Exposure and PRECAUTIONS , Hemodialysis ).
CONTRAINDICATIONS
Fosinopril sodium tablets are contraindicated in patients who are hypersensitive to this product or to any other angiotensin-converting enzyme inhibitor (e.g., a patient who has experienced angioedema with any other ACE inhibitor therapy).
Do not co-administer fosinopril sodium tablets with aliskiren in patients with diabetes.
ADVERSE REACTIONS
Fosinopril sodium tablets have been evaluated for safety in more than 2100 individuals in hypertension and heart failure trials, including approximately 530 patients treated for a year or more. Generally adverse events were mild and transient, and their frequency was not prominently related to dose within the recommended daily dosage range.
Hypertension
In placebo-controlled clinical trials (688 fosinopril sodium-treated patients), the usual duration of therapy was 2 to 3 months. Discontinuations due to any clinical or laboratory adverse event were 4.1% and 1.1% in fosinopril sodium-treated and placebo-treated patients, respectively. The most frequent reasons (0.4 to 0.9%) were headache, elevated transaminases, fatigue, cough (see PRECAUTIONS , General , Cough ), diarrhea, and nausea and vomiting.
During clinical trials with any fosinopril sodium regimen, the incidence of adverse events in the elderly (≥ 65 years old) was similar to that seen in younger patients.
Clinical adverse events probably or possibly related or of uncertain relationship to therapy, occurring in at least 1% of patients treated with fosinopril sodium alone and at least as frequent on fosinopril sodium as on placebo in placebo-controlled clinical trials are shown in the table below.
| Fosinopril Sodium (N = 688) Incidence (Discontinuation) | Placebo (N = 184) Incidence (Discontinuation) | |
|---|---|---|
Cough | 2.2 (0.4) | 0.0 (0.0) |
Dizziness | 1.6 (0.0) | 0.0 (0.0) |
Nausea/Vomiting | 1.2 (0.4) | 0.5 (0.0) |
The following events were also seen at > 1% on fosinopril sodium but occurred in the placebo group at a greater rate: headache, diarrhea, fatigue, and sexual dysfunction. Other clinical events probably or possibly related, or of uncertain relationship to therapy occurring in 0.2 to 1.0% of patients (except as noted) treated with fosinopril sodium in controlled or uncontrolled clinical trials (N = 1479) and less frequent, clinically significant events include (listed by body system):
General: Chest pain, edema, weakness, excessive sweating.
Cardiovascular: Angina/myocardial infarction, cerebrovascular accident, hypertensive crisis, rhythm disturbances, palpitations, hypotension, syncope, flushing, claudication.
Orthostatic hypotension occurred in 1.4% of patients treated with fosinopril monotherapy. Hypotension or orthostatic hypotension was a cause for discontinuation of therapy in 0.1% of patients.
Dermatologic: Urticaria, rash, photosensitivity, pruritus.
Endocrine/Metabolic: Gout, decreased libido.
Gastrointestinal: Pancreatitis, hepatitis, dysphagia, abdominal distention, abdominal pain, flatulence, constipation, heartburn, appetite/weight change, dry mouth.
Hematologic: Lymphadenopathy.
Immunologic: Angioedema (see WARNINGS , Head and Neck Angioedema and Intestinal Angioedema ).
Musculoskeletal: Arthralgia, musculoskeletal pain, myalgia/muscle cramp.
Nervous/Psychiatric: Memory disturbance, tremor, confusion, mood change, paresthesia, sleep disturbance, drowsiness, vertigo.
Respiratory: Bronchospasm, pharyngitis, sinusitis/rhinitis, laryngitis/hoarseness, epistaxis. A symptom-complex of cough, bronchospasm, and eosinophilia has been observed in two patients treated with fosinopril.
Special Senses: Tinnitus, vision disturbance, taste disturbance, eye irritation.
Urogenital: Renal insufficiency, urinary frequency.
Heart Failure
In placebo-controlled clinical trials (361 fosinopril sodium-treated patients), the usual duration of therapy was 3 to 6 months. Discontinuations due to any clinical or laboratory adverse event, except for heart failure, were 8.0% and 7.5% in fosinopril sodium-treated and placebo-treated patients, respectively. The most frequent reason for discontinuation of fosinopril sodium was angina pectoris (1.1%). Significant hypotension after the first dose of fosinopril sodium occurred in 14/590 (2.4%) of patients; 5/590 (0.8%) patients discontinued due to first dose hypotension.
Clinical adverse events probably or possibly related or of uncertain relationship to therapy, occurring in at least 1% of patients treated with fosinopril sodium and at least as common as the placebo group, in placebo-controlled trials are shown in the table below.
| Fosinopril Sodium (N = 361) Incidence (Discontinuation) | Placebo (N = 373) Incidence (Discontinuation) | |
|---|---|---|
Dizziness | 11.9 (0.6) | 5.4 (0.3) |
Cough | 9.7 (0.8) | 5.1 (0.0) |
Hypotension | 4.4 (0.8) | 0.8 (0.0) |
Musculoskeletal Pain | 3.3 (0.0) | 2.7 (0.0) |
Nausea/Vomiting | 2.2 (0.6) | 1.6 (0.3) |
Diarrhea | 2.2 (0.0) | 1.3 (0.0) |
Chest Pain (non-cardiac) | 2.2 (0.0) | 1.6 (0.0) |
Upper Respiratory Infection | 2.2 (0.0) | 1.3 (0.0) |
Orthostatic Hypotension | 1.9 (0.0) | 0.8 (0.0) |
Subjective Cardiac Rhythm Disturbance | 1.4 (0.6) | 0.8 (0.3) |
Weakness | 1.4 (0.3) | 0.5 (0.0) |
The following events also occurred at a rate of 1% or more on fosinopril sodium tablets but occurred on placebo more often: fatigue, dyspnea, headache, rash, abdominal pain, muscle cramp, angina pectoris, edema, and insomnia.
The incidence of adverse events in the elderly (≥ 65 years old) was similar to that seen in younger patients.
Other clinical events probably or possibly related, or of uncertain relationship to therapy occurring in 0.4 to 1.0% of patients (except as noted) treated with fosinopril sodium in controlled clinical trials (N = 516) and less frequent, clinically significant events include (listed by body system):
General: Fever, influenza, weight gain, hyperhidrosis, sensation of cold, fall, pain.
Cardiovascular: Sudden death, cardiorespiratory arrest, shock (0.2%), atrial rhythm disturbance, cardiac rhythm disturbances, non-anginal chest pain, edema lower extremity, hypertension, syncope, conduction disorder, bradycardia, tachycardia.
Dermatologic: Pruritus.
Endocrine/Metabolic: Gout, sexual dysfunction.
Gastrointestinal: Hepatomegaly, abdominal distention, decreased appetite, dry mouth, constipation, flatulence.
Immunologic: Angioedema (0.2%).
Musculoskeletal: Muscle ache, swelling of an extremity, weakness of an extremity.
Nervous/Psychiatric: Cerebral infarction, TIA, depression, numbness, paresthesia, vertigo, behavior change, tremor.
Respiratory: Abnormal vocalization, rhinitis, sinus abnormality, tracheobronchitis, abnormal breathing, pleuritic chest pain.
Special Senses: Vision disturbance, taste disturbance.
Urogenital: Abnormal urination, kidney pain.
Potential Adverse Effects Reported With ACE Inhibitors
Body as a whole: Anaphylactoid reactions (see WARNINGS , Anaphylactoid and Possibly Related Reactions and PRECAUTIONS , Hemodialysis ).
Other medically important adverse effects reported with ACE inhibitors include: Cardiac arrest; eosinophilic pneumonitis; neutropenia/agranulocytosis, pancytopenia, anemia (including hemolytic and aplastic), thrombocytopenia; acute renal failure; hepatic failure, jaundice (hepatocellular or cholestatic); symptomatic hyponatremia; bullous pemphigus, exfoliative dermatitis; a syndrome which may include: arthralgia/arthritis, vasculitis, serositis, myalgia, fever, rash or other dermatologic manifestations, a positive ANA, leukocytosis, eosinophilia, or an elevated ESR.
Laboratory Test Abnormalities
Serum Electrolytes
Hyperkalemia, (see PRECAUTIONS ); hyponatremia, (see PRECAUTIONS , Drug Interactions , Diuretics ).
BUN/Serum Creatinine
Elevations, usually transient and minor, of BUN or serum creatinine have been observed. In placebo-controlled clinical trials, there were no significant differences in the number of patients experiencing increases in serum creatinine (outside the normal range or 1.33 times the pre-treatment value) between the fosinopril and placebo treatment groups. Rapid reduction of longstanding or markedly elevated blood pressure by any antihypertensive therapy can result in decreases in the glomerular filtration rate, and in turn, lead to increases in BUN or serum creatinine (see PRECAUTIONS , General ).
Hematology
In controlled trials, a mean hemoglobin decrease of 0.1 g/dL was observed in fosinopril-treated patients. In individual patients decreases in hemoglobin or hematocrit were usually transient, small, and not associated with symptoms. No patient was discontinued from therapy due to the development of anemia. Other: Neutropenia (see WARNINGS ), leukopenia and eosinophilia.
Liver Function Tests
Elevations of transaminases, LDH, alkaline phosphatase, and serum bilirubin have been reported. Fosinopril therapy was discontinued because of serum transaminase elevations in 0.7% of patients. In the majority of cases, the abnormalities were either present at baseline or were associated with other etiologic factors. In those cases which were possibly related to fosinopril therapy, the elevations were generally mild and transient and resolved after discontinuation of therapy.
Pediatric Patients
The adverse experience profile for pediatric patients is similar to that seen in adult patients with hypertension. The long-term effects of fosinopril sodium on growth and development have not been studied.
Drug Interactions
Diuretics
Patients on diuretics, especially those with intravascular volume depletion, may occasionally experience an excessive reduction of blood pressure after initiation of therapy with fosinopril sodium tablets. The possibility of hypotensive effects with fosinopril sodium can be minimized by either discontinuing the diuretic or increasing salt intake prior to initiation of treatment with fosinopril sodium. If this is not possible, the starting dose should be reduced and the patient should be observed closely for several hours following an initial dose and until blood pressure has stabilized (see DOSAGE AND ADMINISTRATION ).
Agents increasing serum potassium
Coadministration of fosinopril with potassium sparing diuretics, potassium supplements, potassium-containing salt substitutes or other drugs that raise serum potassium levels may result in hyperkalemia. Monitor serum potassium in such patients.
Lithium
Increased serum lithium levels and symptoms of lithium toxicity have been reported in patients receiving ACE inhibitors during therapy with lithium. These drugs should be coadministered with caution, and frequent monitoring of serum lithium levels is recommended. If a diuretic is also used, the risk of lithium toxicity may be increased.
Antacids
In a clinical pharmacology study, coadministration of an antacid (aluminum hydroxide, magnesium hydroxide, and simethicone) with fosinopril reduced serum levels and urinary excretion of fosinoprilat as compared with fosinopril administrated alone, suggesting that antacids may impair absorption of fosinopril. Therefore, if concomitant administration of these agents is indicated, dosing should be separated by 2 hours.
Gold
Nitritoid reactions (symptoms include facial flushing, nausea, vomiting, and hypotension) have been reported rarely in patients on therapy with injectable gold (sodium aurothiomalate) and concomitant ACE inhibitor therapy including fosinopril sodium.
Non-steroidal anti-inflammatory agents including selective cyclooxygenase-2 inhibitors (COX-2 inhibitors)
In patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, co-administration of NSAIDs, including selective COX-2 inhibitors, with ACE inhibitors, including fosinopril, may result in deterioration of renal function, including possible acute renal failure. These effects are usually reversible. Monitor renal function periodically in patients receiving quinapril and NSAID therapy.
The antihypertensive effect of ACE inhibitors, including fosinopril may be attenuated by NSAIDs.
Agents that inhibit mTOR
Patients taking concomitant mTOR inhibitor (e.g. temsirolimus) therapy may be at increased risk for angioedema.
Dual Blockade of the Renin-Angiotensin System (RAS)
Dual blockade of the RAS with angiotensin receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Most patients receiving the combination of two RAS inhibitors do not obtain any additional benefit compared to monotherapy. In general, avoid combined use of RAS inhibitors. Closely monitor blood pressure, renal function and electrolytes in patients on fosinopril and other agents that affect the RAS.
Do not co-administer aliskiren with fosinopril in patients with diabetes. Avoid concomitant use of aliskiren with fosinopril in patients with renal impairment (GFR<60 mL/min/1.73 m 2 ).
Other
Neither fosinopril sodium nor its metabolites have been found to interact with food. In separate single or multiple dose pharmacokinetic interaction studies with chlorthalidone, nifedipine, propranolol, hydrochlorothiazide, cimetidine, metoclopramide, propantheline, digoxin, and warfarin, the bioavailability of fosinoprilat was not altered by coadministration of fosinopril with any one of these drugs. In a study with concomitant administration of aspirin and fosinopril sodium, the bioavailability of unbound fosinoprilat was not altered.
In a pharmacokinetic interaction study with warfarin, bioavailability parameters, the degree of protein binding, and the anticoagulant effect (measured by prothrombin time) of warfarin were not significantly changed.
DESCRIPTION
Fosinopril sodium is the sodium salt of fosinopril, the ester prodrug of an angiotensin-converting enzyme (ACE) inhibitor, fosinoprilat. It contains a phosphinate group capable of specific binding to the active site of angiotensin-converting enzyme. Fosinopril sodium is designated chemically as: L-proline, 4-cyclohexyl-1-[[[2-methyl-1-(1-oxopropoxy) propoxy] (4-phenylbutyl) phosphinyl] acetyl]-, sodium salt, trans- .
Fosinopril sodium is a white to off-white crystalline powder. It is soluble in water (100 mg/mL), methanol, and ethanol and slightly soluble in hexane.
Its structural formula is:
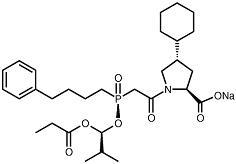
C 30 H 45 NNaO 7 P M.W. 585.65
Fosinopril sodium, USP, is available for oral administration as 10 mg, 20 mg, and 40 mg tablets. Inactive ingredients include: crospovidone, lactose monohydrate, microcrystalline cellulose, povidone, and sodium stearyl fumarate.
CLINICAL PHARMACOLOGY
Mechanism of Action
In animals and humans, fosinopril sodium is hydrolyzed by esterases to the pharmacologically active form, fosinoprilat, a specific competitive inhibitor of angiotensin-converting enzyme (ACE).
ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. The latter decrease may result in a small increase of serum potassium.
In 647 hypertensive patients treated with fosinopril alone for an average of 29 weeks, mean increases in serum potassium of 0.1 mEq/L were observed. Similar increases were observed among all patients treated with fosinopril, including those receiving concomitant diuretic therapy. Removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of fosinopril sodium remains to be elucidated.
While the mechanism through which fosinopril sodium lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, fosinopril sodium has an antihypertensive effect even in patients with low-renin hypertension. Although fosinopril sodium was antihypertensive in all races studied, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to ACE inhibitor monotherapy than non-black patients.
In patients with heart failure, the beneficial effects of fosinopril sodium are thought to result primarily from suppression of the renin-angiotensin-aldosterone system; inhibition of the angiotensin-converting enzyme produces decreases in both preload and afterload.
Pharmacokinetics and Metabolism
Following oral administration, fosinopril (the prodrug) is absorbed slowly. The absolute absorption of fosinopril averaged 36% of an oral dose. The primary site of absorption is the proximal small intestine (duodenum/jejunum). While the rate of absorption may be slowed by the presence of food in the gastrointestinal tract, the extent of absorption of fosinopril is essentially unaffected.
Fosinoprilat is highly protein-bound (approximately 99.4%), has a relatively small volume of distribution, and has negligible binding to cellular components in blood. After single and multiple oral doses, plasma levels, areas under plasma concentration-time curves (AUCs) and peak concentrations (C maxs ) are directly proportional to the dose of fosinopril. Times to peak concentrations are independent of dose and are achieved in approximately 3 hours.
After an oral dose of radiolabeled fosinopril, 75% of radioactivity in plasma was present as active fosinoprilat, 20 to 30% as a glucuronide conjugate of fosinoprilat, and 1 to 5% as a p -hydroxy metabolite of fosinoprilat. Since fosinoprilat is not biotransformed after intravenous administration, fosinopril, not fosinoprilat, appears to be the precursor for the glucuronide and p -hydroxy metabolites. In rats, the p -hydroxy metabolite of fosinoprilat is as potent an inhibitor of ACE as fosinoprilat; the glucuronide conjugate is devoid of ACE inhibitory activity.
After intravenous administration, fosinoprilat was eliminated approximately equally by the liver and kidney. After oral administration of radiolabeled fosinopril, approximately half of the absorbed dose is excreted in the urine and the remainder is excreted in the feces. In two studies involving healthy subjects, the mean body clearance of intravenous fosinoprilat was between 26 and 39 mL/min.
In healthy subjects, the terminal elimination half-life (t 1/2 ) of an intravenous dose of radiolabeled fosinoprilat is approximately 12 hours. In hypertensive patients with normal renal and hepatic function, who received repeated doses of fosinopril, the effective t 1/2 for accumulation of fosinoprilat averaged 11.5 hours. In patients with heart failure, the effective t 1/2 was 14 hours.
In patients with mild to severe renal insufficiency (creatinine clearance 10 to 80 mL/min/1.73 m 2 ), the clearance of fosinoprilat does not differ appreciably from normal, because of the large contribution of hepatobiliary elimination. In patients with end-stage renal disease (creatinine clearance < 10 mL/min/1.73 m 2 ), the total body clearance of fosinoprilat is approximately one-half of that in patients with normal renal function (see DOSAGE AND ADMINISTRATION ).
Fosinopril is not well dialyzed. Clearance of fosinoprilat by hemodialysis and peritoneal dialysis averages 2% and 7%, respectively, of urea clearances.
In patients with hepatic insufficiency (alcoholic or biliary cirrhosis) , the extent of hydrolysis of fosinopril is not appreciably reduced, although the rate of hydrolysis may be slowed; the apparent total body clearance of fosinoprilat is approximately one-half of that in patients with normal hepatic function.
In elderly (male) subjects (65 to 74 years old) with clinically normal renal and hepatic function, there appear to be no significant differences in pharmacokinetic parameters for fosinoprilat compared to those of younger subjects (20 to 35 years old).
In pediatric patients , (N = 20) age 6 to 16 years, with glomerular filtration rate ≥ 25 mL/min, given a single dose of fosinopril (0.3 mg/kg given as solution), the mean AUC and C max values of fosinoprilat (the active form of fosinopril) were similar to those seen in healthy adults receiving 20 mg (about 0.3 mg/kg for a 70 kg adult) of fosinopril as a solution. The terminal elimination half-life of fosinoprilat in pediatric patients was 11 to 13 hours, also similar to that observed in adults.
Fosinoprilat was found to cross the placenta of pregnant animals.
Studies in animals indicate that fosinopril and fosinoprilat do not cross the blood-brain barrier.
Pharmacodynamics and Clinical Effects
Serum ACE activity was inhibited by ≥ 90% at 2 to 12 hours after single doses of 10 to 40 mg of fosinopril. At 24 hours, serum ACE activity remained suppressed by 85%, 93%, and 93% in the 10, 20, and 40 mg dose groups, respectively.
Hypertension
Adult
Administration of fosinopril sodium tablets to patients with mild to moderate hypertension results in a reduction of both supine and standing blood pressure to about the same extent with no compensatory tachycardia. Symptomatic postural hypotension is infrequent, although it can occur in patients who are salt- and/or volume-depleted (see WARNINGS ). Use of fosinopril sodium in combination with thiazide diuretics gives a blood pressure-lowering effect greater than that seen with either agent alone.
Following oral administration of single doses of 10 to 40 mg, fosinopril sodium lowered blood pressure within 1 hour, with peak reductions achieved 2 to 6 hours after dosing. The antihypertensive effect of a single dose persisted for 24 hours. Following 4 weeks of monotherapy in placebo-controlled trials in patients with mild to moderate hypertension, once daily doses of 20 to 80 mg lowered supine or seated systolic and diastolic blood pressures 24 hours after dosing by an average of 8 to 9/6 to 7 mmHg more than placebo. The trough effect was about 50 to 60% of the peak diastolic response and about 80% of the peak systolic response.
In most trials, the antihypertensive effect of fosinopril sodium increased during the first several weeks of repeated measurements. The antihypertensive effect of fosinopril sodium has been shown to continue during long-term therapy for at least 2 years. Abrupt withdrawal of fosinopril sodium has not resulted in a rapid increase in blood pressure.
Limited experience in controlled and uncontrolled trials combining fosinopril with a calcium channel blocker or a loop diuretic has indicated no unusual drug-drug interactions. Other ACE inhibitors have had less than additive effects with beta-adrenergic blockers, presumably because both drugs lower blood pressure by inhibiting parts of the renin-angiotensin system.
ACE inhibitors are generally less effective in blacks than in non-blacks. The effectiveness of fosinopril sodium was not influenced by age, sex, or weight.
In hemodynamic studies in hypertensive patients, after 3 months of therapy, responses (changes in BP, heart rate, cardiac index, and PVR) to various stimuli (e.g., isometric exercise, 45° head-up tilt, and mental challenge) were unchanged compared to baseline, suggesting that fosinopril sodium does not affect the activity of the sympathetic nervous system. Reduction in systemic blood pressure appears to have been mediated by a decrease in peripheral vascular resistance without reflex cardiac effects. Similarly, renal, splanchnic, cerebral, and skeletal muscle blood flow were unchanged compared to baseline, as was glomerular filtration rate.
Pediatric
Reduction of blood pressure with low (0.1 mg/kg), medium (0.3 mg/kg) and high (0.6 mg/kg) target doses of once-daily fosinopril was evaluated in a randomized, double-blind study of 252 pediatric patients 6 to 16 years of age with hypertension or high-normal blood pressure. Fosinopril doses in the medium and high dose groups were titrated to target doses after 1 week and the total duration of treatment was 4 weeks. The maximum dose studied was 40 mg once daily. At the end of 4 weeks of treatment, the mean reductions from baseline in trough systolic blood pressure were similar in all three dose groups. Withdrawal of fosinopril treatment resulted in an increase in blood pressure towards baseline over a 2 week period. Fosinopril was generally well tolerated.
Heart Failure
In a randomized, double-blind, placebo-controlled trial, 179 patients with heart failure, all receiving diuretics and some receiving digoxin, were administered single doses of 10, 20, or 40 mg of fosinopril sodium or placebo. Doses of 20 and 40 mg of fosinopril sodium resulted in acute decreases in pulmonary capillary wedge pressure (preload) and mean arterial blood pressure and systemic vascular resistance (afterload). One hundred fifty-five of these patients were re-randomized to once daily therapy with fosinopril sodium (10, 20, or 40 mg) for an additional 10 weeks. Hemodynamic measurements made 24 hours after dosing showed (relative to baseline) continued reduction in pulmonary capillary wedge pressure, mean arterial blood pressure, right atrial pressure and an increase in cardiac index and stroke volume for the 20 and 40 mg dose groups. No tachyphylaxis was seen.
Fosinopril sodium was studied in 3 double-blind, placebo-controlled, 12 to 24 week trials including a total of 734 patients with heart failure, with fosinopril sodium doses from 10 to 40 mg daily. Concomitant therapy in 2 of these 3 trials included diuretics and digitalis; in the third trial patients were receiving only diuretics. All 3 trials showed statistically significant benefits of fosinopril sodium therapy, compared to placebo, in one or more of the following: exercise tolerance (1 study), symptoms of dyspnea, orthopnea and paroxysmal nocturnal dyspnea (2 studies), NYHA classification (2 studies), hospitalization for heart failure (2 studies), study withdrawals for worsening heart failure (2 studies), and/or need for supplemental diuretics (2 studies). Favorable effects were maintained for up to 2 years. Effects of fosinopril sodium on long-term mortality in heart failure have not been evaluated. The once daily dosage for the treatment of congestive heart failure was the only dosage regimen used during clinical trial development and was determined by the measurement of hemodynamic responses.
HOW SUPPLIED
Fosinopril sodium tablets USP, 10 mg: White to off-white, capsule-shaped tablets, both sides scored, debossed with “S|10” on one side and “|” on the other side. They are supplied in bottles of 90 (NDC 43547-386-09) and 1000 (NDC 43547-386-11).
Fosinopril sodium tablets USP, 20 mg: White to off-white, round tablets debossed with “S 20” on one side and plain on the other side. They are supplied in bottles of 90 (NDC 43547-387-09) and 1000 (NDC 43547-387-11).
Fosinopril sodium tablets USP, 40 mg: White to off-white, round tablets debossed with “S 40” on one side and plain on the other side. They are supplied in bottles of 90 (NDC 43547-388-09) and 1000 (NDC 43547-388-11).
Mechanism of Action
In animals and humans, fosinopril sodium is hydrolyzed by esterases to the pharmacologically active form, fosinoprilat, a specific competitive inhibitor of angiotensin-converting enzyme (ACE).
ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. The latter decrease may result in a small increase of serum potassium.
In 647 hypertensive patients treated with fosinopril alone for an average of 29 weeks, mean increases in serum potassium of 0.1 mEq/L were observed. Similar increases were observed among all patients treated with fosinopril, including those receiving concomitant diuretic therapy. Removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of fosinopril sodium remains to be elucidated.
While the mechanism through which fosinopril sodium lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, fosinopril sodium has an antihypertensive effect even in patients with low-renin hypertension. Although fosinopril sodium was antihypertensive in all races studied, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to ACE inhibitor monotherapy than non-black patients.
In patients with heart failure, the beneficial effects of fosinopril sodium are thought to result primarily from suppression of the renin-angiotensin-aldosterone system; inhibition of the angiotensin-converting enzyme produces decreases in both preload and afterload.