Floxuridine - Floxuridine injection, Powder, Lyophilized, For Solution prescribing information
WARNING
It is recommended that floxuridine be given only by or under the supervision of a qualified physician who is experienced in cancer chemotherapy and intra-arterial drug therapy and is well versed in the use of potent antimetabolites.
Because of the possibility of severe toxic reactions, all patients should be hospitalized for initiation of the first course of therapy.
INDICATIONS AND USAGE
Floxuridine for Injection, USP is effective in the palliative management of gastrointestinal adenocarcinoma metastatic to the liver, when given by continuous regional intra-arterial infusion in carefully selected patients who are considered incurable by surgery or other means. Patients with known disease extending beyond an area capable of infusion via a single artery should, except in unusual circumstances, be considered for systemic therapy with other chemotherapeutic agents.
DOSAGE AND ADMINISTRATION
Each vial must be reconstituted with 5 mL of sterile water for injection to yield a solution containing approximately 100 mg of floxuridine/mL. The calculated daily dose(s) of the drug is then diluted with 5% dextrose or 0.9% sodium chloride injection to a volume appropriate for the infusion apparatus to be used. The administration of floxuridine is best achieved with the use of an appropriate pump to overcome pressure in large arteries and to ensure a uniform rate of infusion.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit.
The recommended therapeutic dosage schedule of floxuridine by continuous arterial infusion is 0.1 to 0.6 mg/kg/day. The higher dosage ranges (0.4 to 0.6 mg) are usually employed for hepatic artery infusion because the liver metabolizes the drug, thus reducing the potential for systemic toxicity.
Therapy can be given until adverse reactions appear. (See PRECAUTIONS section.) When these side effects have subsided, therapy may be resumed. The patient should be maintained on therapy as long as response to floxuridine continues.
Procedures for proper handling and disposal of anticancer drugs should be considered. Several guidelines on this subject have been published. 1-7 There is no general agreement that all of the procedures recommended in the guidelines are necessary or appropriate.
CONTRAINDICATIONS
Floxuridine therapy is contraindicated for patients in a poor nutritional state, those with depressed bone marrow function or those with potentially serious infections.
ADVERSE REACTIONS
Adverse reactions to the arterial infusion of floxuridine are generally related to the procedural complications of regional arterial infusion.
The more common adverse reactions to the drug are nausea, vomiting, diarrhea, enteritis, stomatitis and localized erythema. The more common laboratory abnormalities are anemia, leukopenia, thrombo-cytopenia and elevations of alkaline phosphatase, serum transaminase, serum bilirubin and lactic dehydrogenase.
Other adverse reactions are:
Gastrointestinal: duodenal ulcer, duodenitis, gastritis, bleeding, gastroenteritis, glossitis, pharyngitis, anorexia, cramps, abdominal pain; possible intra- and extrahepatic biliary sclerosis, as well as acalculous cholecystitis.
Dermatologic: alopecia, dermatitis, nonspecific skin toxicity, rash.
Cardiovascular: myocardial ischemia.
Miscellaneous Clinical Reactions: fever, lethargy, malaise, weakness.
Laboratory Abnormalities: BSP, prothrombin, total proteins, sedimentation rate and thrombopenia.
Procedural Complications of Regional Arterial Infusion: arterial aneurysm; arterial ischemia; arterial thrombosis; embolism; fibromyositis; thrombophlebitis; hepatic necrosis; abscesses; infection at catheter site; bleeding at catheter site; catheter blocked, displaced or leaking.
The following adverse reactions have not been reported with floxuridine but have been noted following the administration of 5-fluorouracil. While the possibility of these occurring following floxuridine therapy is remote because of its regional administration, one should be alert for these reactions following the administration of floxuridine because of the pharmacological similarity of these two drugs: pancytopenia, agranulocytosis, myocardial ischemia, angina, anaphylaxis, generalized allergic reactions, acute cerebellar syndrome, nystagmus, headache, dry skin, fissuring, photosensitivity, pruritic maculopapular rash, increased pigmentation of the skin, vein pigmentation, lacrimal duct stenosis, visual changes, lacrimation, photophobia, disorientation, confusion, euphoria, epistaxis and nail changes, including loss of nails.
Drug Interactions
See WARNINGS section.
DESCRIPTION
Floxuridine for Injection, USP, an antineoplastic antimetabolite, is available as a sterile, nonpyrogenic, lyophilized powder for reconstitution. Each vial contains 500 mg of floxuridine which is to be reconstituted with 5 mL of sterile water for injection. An appropriate amount of reconstituted solution is then diluted with a parenteral solution for intra-arterial infusion (see DOSAGE AND ADMINISTRATION section).
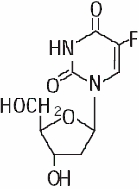
Floxuridine is a fluorinated pyrimidine. Chemically, floxuridine is 2'-Deoxy-5-fluorouridine, with a molecular formula of C 9 H 11 FN 2 O 5 . It is a white to off-white odorless solid which is freely soluble in water.
The 2% aqueous solution has a pH of between 4.0 and 5.5. The molecular weight of floxuridine is 246.20 and the structural formula is:
CLINICAL PHARMACOLOGY
When floxuridine is given by rapid intra-arterial injection it is apparently rapidly catabolized to 5-fluorouracil. Thus, rapid injection of floxuridine produces the same toxic and antimetabolic effects as does 5-fluorouracil. The primary effect is to interfere with the synthesis of deoxyribonucleic acid (DNA) and to a lesser extent inhibit the formation of ribonucleic acid (RNA). However, when floxuridine is given by continuous intra-arterial infusion its direct anabolism to floxuridine-monophosphate is enhanced, thus increasing the inhibition of DNA.
Floxuridine is metabolized in the liver. The drug is excreted intact and as urea, fluorouracil, a-fluoro-b-ureidopropionic acid, dihydrofluorouracil, a-fluoro-b-guanidopropionic acid and a-fluoro-b-alanine in the urine; it is also expired as respiratory carbon dioxide. Pharmacokinetic data on intra-arterial infusion of floxuridine are not available.
HOW SUPPLIED
Floxuridine for Injection, USP, 500 mg, lyophilized, in a 5 mL vial, is supplied in individual cartons.
NDC 81643-9270-1. This is to be reconstituted with 5 mL sterile water for injection. The sterile powder should be stored at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature]. Reconstituted vials should be stored under refrigeration 2° to 8°C (36° to 46°F) for not more than 2 weeks.
To report SUSPECTED ADVERSE REACTIONS, contact Hikma Pharmaceuticals USA Inc. at 1-877-845-0689, or the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
For Product Inquiry call 1-877-845-0689.