Get your patient on Endari - Glutamine powder, For Solution (Glutamine)
Endari - Glutamine powder, For Solution prescribing information
INDICATIONS AND USAGE
Endari is indicated to reduce the acute complications of sickle cell disease in adult and pediatric patients 5 years of age and older.
DOSAGE AND ADMINISTRATION
Dosage
Administer Endari orally, twice per day at the dose based on body weight according to Table 1.
| Weight in kilograms | Weight in pounds | Per dose in grams | Per day in grams | Packets per dose | Packets per day |
|---|---|---|---|---|---|
| less than 30 | less than 66 | 5 | 10 | 1 | 2 |
| 30 to 65 | 66 to 143 | 10 | 20 | 2 | 4 |
| greater than 65 | greater than 143 | 15 | 30 | 3 | 6 |
Preparation of Product
Mix Endari immediately before ingestion with 8 oz. (240 mL) of cold or room temperature beverage, such as water, milk or apple juice, or 4 oz. to 6 oz. of food such as applesauce or yogurt. Complete dissolution is not required prior to administration.
DOSAGE FORMS AND STRENGTHS
Oral powder: 5 grams of L–glutamine as a white crystalline powder in paper-foil-plastic laminate packets
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are no available data on Endari use in pregnant women to inform a drug-associated risk of major birth defects and miscarriage. Animal reproduction studies were not conducted with Endari.
Adverse outcomes in pregnancy occur regardless of the health of the mother or the use of medications. The background risk of major birth defects and miscarriage for the indicated population are unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Lactation
Risk Summary
There are no data on the presence of Endari in human milk, the effect on the breastfed infant or the effect on milk production. The developmental and health benefits from breastfeeding should be considered along with the mother's clinical need for Endari and any potential adverse effects on the breastfed child from Endari or from the underlying maternal condition.
Pediatric Use
The safety and effectiveness of Endari have been established in pediatric patients 5 years and older. Use of Endari is supported by evidence from 2 placebo-controlled studies in adult and pediatric patients with sickle cell disease. The clinical studies enrolled 110 pediatric patients in the following age groups: 46 children (5 years up to less than 12 years) and 64 adolescents (12 years to less than 17 years).
The safety and effectiveness of Endari in pediatric patients with sickle cell disease younger than 5 years old has not been established.
Geriatric Use
Clinical studies of Endari did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
CONTRAINDICATIONS
None
ADVERSE REACTIONS
Most common adverse reactions (incidence > 10%) are constipation, nausea, headache, abdominal pain, cough, pain in extremity, back pain, and chest pain. (6 )
To report SUSPECTED ADVERSE REACTIONS, contact Emmaus Medical, Inc. at 1-877-420-6493 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described below reflect exposure to Endari in 187 patients, including 136 exposed for 6 months and 109 exposed for ≥1 year. Endari was studied in 2 placebo-controlled clinical trials (a phase 3 study, n=230 and a phase 2 study, n=70). In these trials, patients with sickle cell anemia or sickle β 0 -thalassemia were randomized to receive Endari (n=187) or placebo (n=111) orally twice daily for 48 weeks followed by 3 weeks of tapering. Both studies included pediatric and adult patients (5-58 years of age) and 54% were female. The majority of patients were black (97.3%), had a diagnosis of sickle cell anemia (89.9%) and were receiving hydroxyurea at baseline (63.4%).
Treatment discontinuation due to adverse reactions was reported in 2.7% (n=5) of patients receiving Endari. These adverse reactions included one case each of hypersplenism, abdominal pain, dyspepsia, burning sensation, and hot flash.
Serious adverse reactions were reported in both treatment groups, more frequently in the placebo group, and were consistent with the underlying disease.
Three deaths (3/187=1.6%) occurred during the study in the Endari treatment group as compared to none in the placebo treatment group. None of the deaths were considered to be related to Endari treatment. Adverse reactions occurring in greater than 10% of patients treated with Endari are shown in Table 2 below.
| Adverse reaction | Endari N = 187 (%) | Placebo N = 111 (%) |
|---|---|---|
| Constipation | 21 | 18 |
| Nausea | 19 | 14 |
| Headache | 18 | 15 |
| Abdominal Pain Abdominal pain = abdominal pain and abdominal pain, upper | 17 | 16 |
| Cough | 16 | 14 |
| Pain in extremity | 13 | 7 |
| Back pain | 12 | 5 |
| Chest pain | 12 | 8 |
Drug Interactions
No drug interaction studies have been conducted.
DESCRIPTION
Endari (L-glutamine) is an amino acid. L-glutamine is designated chemically as (S)-2-aminoglutaramic acid, L-glutamic acid 5-amide, or (S)-2,5-diamino-5-oxopentanoic acid. The molecular formula is C 5 H 10 N 2 O 3 with the molecular weight of 146.15 g/mol and the following structural formula:
Endari is formulated as a white crystalline powder and is packaged as 5 grams in a paper-foil-plastic laminate packet for oral administration.
CLINICAL PHARMACOLOGY
Mechanism of Action
The mechanism of action of the amino acid L-glutamine in treating sickle cell disease (SCD) is not fully understood. Oxidative stress phenomena are involved in the pathophysiology of SCD. Sickle red blood cells (RBCs) are more susceptible to oxidative damage than normal RBCs, which may contribute to the chronic hemolysis and vaso-occlusive events associated with SCD. The pyridine nucleotides, NAD + and its reduced form NADH, play roles in regulating and preventing oxidative damage in RBCs. L-glutamine may improve the NAD redox potential in sickle RBCs through increasing the availability of reduced glutathione.
Pharmacodynamics
In vivo analyses demonstrated that L-glutamine supplementation improved NAD redox potential.
Pharmacokinetics
The pharmacokinetics of L-glutamine has been studied in healthy subjects and a variety of disease states. Relevant results from published literature are summarized below.
Absorption
Following single-dose oral administration of L-glutamine at 0.1 g/kg, mean peak L-glutamine concentration was 1028 µM (or 150 mcg/mL) occurring approximately 30 minutes after administration.
The pharmacokinetics following multiple oral doses at 0.1 g/kg, 0.3 g/kg, and 0.6 g/kg found peak concentrations increasing with each dose, but maximum concentration did not increase proportionally to the dose, suggesting a saturable absorption process. The peak concentration was seen occurring approximately one hour after administration. There was no accumulation of L-glutamine levels upon multiple oral doses administered twice-daily.
Effect of Food
No significant change in L-glutamine concentration was associated with food, suggesting that L-glutamine can be taken with or without food.
Distribution
After multiple oral doses, the apparent volume of distribution was estimated to be approximately 750 mL/kg.
Elimination
After an intravenous bolus dose, the terminal elimination half-life of L-glutamine was approximately one hour.
Metabolism
Endogenous L-glutamine participates in various metabolic activities, including the formation of glutamate, and synthesis of proteins, nucleotides, and amino sugars. Exogenous L-glutamine is anticipated to undergo similar metabolism.
Excretion
Metabolism is the major route of disappearance for L-glutamine from the plasma. Urinary excretion of L-glutamine was less than 0.3% of the administered dose in intravenous infusion studies.
Specific Populations
In a population pharmacokinetic analysis, body weight was found to be a significant covariate of L-glutamine exposures supporting the tiered body weight based dosing of Endari. The pharmacokinetics of Endari has not been studied in subjects with renal or hepatic impairment.
Drug Interactions
No drug interaction studies have been conducted.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals have not been performed to evaluate the carcinogenic potential of L-glutamine.
L-glutamine was not mutagenic in a bacterial mutagenicity (Ames) assay, nor clastogenic in a chromosome aberration assay in mammalian (Chinese Hamster Lung CHL/IU) cells.
Animal reproduction studies and its potential for impairment of fertility have not been conducted with L-glutamine . It is also not known whether L-glutamine can cause fetal harm when administered to a pregnant woman or whether it can affect reproductive capacity.
Clinical Studies
The efficacy of Endari in sickle cell disease was evaluated in a randomized, double-blind, placebo-controlled, multi-center clinical trial entitled "A Phase III Safety and Efficacy Study of L-Glutamine to Treat Sickle Cell Disease or Sickle β o -thalassemia" [NCT01179217] (see Table 3 ).
The clinical trial evaluated the efficacy and safety of Endari in 230 patients (5 to 58 years of age) with sickle cell anemia or sickle β 0 -thalassemia who had 2 or more painful crises within 12 months prior to enrollment. Eligible patients stabilized on hydroxyurea for at least 3 months continued their therapy throughout the study. The trial excluded patients who had received blood products within 3 weeks, had renal insufficiency or uncontrolled liver disease, or were pregnant (or planning pregnancy) or lactating. Study patients received Endari or placebo for a treatment duration of 48 weeks followed by 3 weeks of tapering. Efficacy was demonstrated by a reduction in the number of sickle cell crises through Week 48 and prior to the start of tapering among patients that received Endari compared to patients who received placebo. This clinical benefit was observed irrespective of hydroxyurea use. A sickle cell crisis was defined as a visit to an emergency room/medical facility for sickle cell disease-related pain which was treated with a parenterally administered narcotic or parenterally administered ketorolac. In addition, the occurrence of chest syndrome, priapism, and splenic sequestration were considered sickle cell crises. Treatment with Endari also resulted in fewer hospitalizations due to sickle cell pain at Week 48, fewer cumulative days in hospital and a lower incidence of acute chest syndrome.
| Event | Endari (n = 152) | Placebo (n = 78) |
|---|---|---|
| Median number of sickle cell crises (min,max) Measured through 48 weeks of treatment | 3 (0, 15) | 4 (0, 15) |
| Median number of hospitalizations for sickle cell pain (min, max) | 2 (0, 14) | 3 (0, 13) |
| Median cumulative days hospitalized (min, max) | 6.5 (0, 94) | 11 (0, 187) |
| Median time (days) to first sickle cell crisis (95% CI) , Hazard Ratio=0.69 (95% CI=0.52, 0.93), estimated based on unstratified Cox's proportional model. Median time and 95% CI were estimated based on the Kaplan Meier method. | 84 (62, 109) | 54 (31, 73) |
| Patients with occurrences of acute chest syndrome (%) | 13 (8.6%) | 18 (23.1%) |
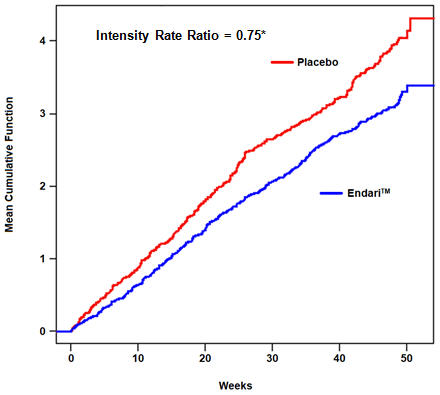
The recurrent crisis event time analysis (Figure 1) yielded an intensity rate ratio (IRR) value of 0.75 with 95% CI= (0.62, 0.90) and (0.55, 1.01) based on unstratified models using the Andersen-Gill and Lin, Wei, Yang and Ying methods, respectively in favor of Endari, suggesting that over the entire 48-week period, the average cumulative crisis count was reduced by 25% from the Endari group over the placebo group.
| Figure 1. Recurrent Event Time for Sickle Cell Crises by Treatment Group | |
| |
| •Andersen-Gill: 95% CI (0.62, 0.90); Lin-Wei-Yang-Ying: 95% CI (0.55, 1.01) | |
HOW SUPPLIED/STORAGE AND HANDLING
Endari is supplied in paper-foil-plastic laminate packets containing 5 grams of L-glutamine white crystalline powder.
- Carton of 60 packets: NDC 42457-420-60
Store at 20°C to 25°C (68°F to 77°F) away from direct sunlight.
Mechanism of Action
The mechanism of action of the amino acid L-glutamine in treating sickle cell disease (SCD) is not fully understood. Oxidative stress phenomena are involved in the pathophysiology of SCD. Sickle red blood cells (RBCs) are more susceptible to oxidative damage than normal RBCs, which may contribute to the chronic hemolysis and vaso-occlusive events associated with SCD. The pyridine nucleotides, NAD + and its reduced form NADH, play roles in regulating and preventing oxidative damage in RBCs. L-glutamine may improve the NAD redox potential in sickle RBCs through increasing the availability of reduced glutathione.