Enalaprilat - Enalaprilat injection prescribing information
USE IN PREGNANCY
When used in pregnancy during the second and third trimesters, ACE inhibitors can cause injury and even death to the developing fetus. When pregnancy is detected, enalaprilat injection should be discontinued as soon as possible. See WARNINGS, Fetal/Neonatal Morbidity and Mortality .
INDICATIONS AND USAGE
Enalaprilat injection is indicated for the treatment of hypertension when oral therapy is not practical.
Enalaprilat injection has been studied with only one other antihypertensive agent, furosemide, which showed approximately additive effects on blood pressure. Enalapril, the pro-drug of enalaprilat, has been used extensively with a variety of other antihypertensive agents, without apparent difficulty except for occasional hypotension.
In using enalaprilat injection, consideration should be given to the fact that another angiotensin-converting enzyme inhibitor, captopril, has caused agranulocytosis, particularly in patients with renal impairment or collagen vascular disease, and that available data are insufficient to show that enalaprilat injection does not have a similar risk (see WARNINGS ).
In considering use of enalaprilat, it should be noted that in controlled clinical trials ACE inhibitors have an effect on blood pressure that is less in black patients than in non-blacks. In addition, it should be noted that black patients receiving ACE inhibitors have been reported to have a higher incidence of angioedema compared to non-blacks (see WARNINGS, Angioedema ).
DOSAGE AND ADMINISTRATION
FOR INTRAVENOUS ADMINISTRATION ONLY
The dose in hypertension is 1.25 mg every six hours administered intravenously over a five minute period. A clinical response is usually seen within 15 minutes. Peak effects after the first dose may not occur for up to four hours after dosing. The peak effects of the second and subsequent doses may exceed those of the first.
No dosage regimen for enalaprilat injection has been clearly demonstrated to be more effective in treating hypertension than 1.25 mg every six hours. However, in controlled clinical studies in hypertension, doses as high as 5 mg every six hours were well tolerated for up to 36 hours. There has been inadequate experience with doses greater than 20 mg per day.
In studies of patients with hypertension, enalaprilat has not been administered for periods longer than 48 hours. In other studies, patients have received enalaprilat for as long as seven days.
The dose for patients being converted to enalaprilat injection from oral therapy for hypertension with enalapril maleate is 1.25 mg every six hours. For conversion from intravenous to oral therapy, the recommended initial dose of oral enalapril maleate, is 5 mg once a day with subsequent dosage adjustments as necessary.
Patients On Diuretic Therapy
For patients on diuretic therapy the recommended starting dose for hypertension is 0.625 mg administered intravenously over a five minute period; also see below, Patients at Risk of Excessive Hypotension. A clinical response is usually seen within 15 minutes. Peak effects after the first dose may not occur for up to four hours after dosing, although most of the effect is usually apparent within the first hour. If after one hour there is an inadequate clinical response, the 0.625 mg dose may be repeated. Additional doses of 1.25 mg may be administered at six hour intervals.
For conversion from intravenous to oral therapy, the recommended initial dose of oral enalapril maleate for patients who have responded to 0.625 mg of enalaprilat every six hours is 2.5 mg once a day with subsequent dosage adjustment as necessary.
Dosage Adjustment in Renal Impairment
The usual dose of 1.25 mg of enalaprilat injection every six hours is recommended for patients with a creatinine clearance > 30 mL/min (serum creatinine of up to approximately 3 mg/dL). For patients with creatinine clearance ≤ 30 mL/min (serum creatinine ≥ 3 mg/dL), the initial dose is 0.625 mg (see WARNINGS ).
If after one hour there is an inadequate clinical response, the 0.625 mg dose may be repeated. Additional doses of 1.25 mg may be administered at six hour intervals.
For dialysis patients, see below, Patients at Risk of Excessive Hypotension .
For conversion from intravenous to oral therapy, the recommended initial dose of oral enalapril maleate is 5 mg once a day for patients with creatinine clearance > 30 mL/min and 2.5 mg once daily for patients with creatinine clearance ≤ 30 mL/min. Dosage should then be adjusted according to blood pressure response.
Patients at Risk of Excessive Hypotension
Hypertensive patients at risk of excessive hypotension include those with the following concurrent conditions or characteristics: heart failure, hyponatremia, high dose diuretic therapy, recent intensive diuresis or increase in diuretic dose, renal dialysis, or severe volume and/or salt depletion of any etiology (see WARNINGS ). Single doses of enalaprilat injection as low as 0.2 mg have produced excessive hypotension in normotensive patients with these diagnoses. Because of the potential for an extreme hypotensive response in these patients, therapy should be started under very close medical supervision. The starting dose should be no greater than 0.625 mg administered intravenously over a period of no less than five minutes and preferably longer (up to one hour).
Patients should be followed closely whenever the dose of enalaprilat injection is adjusted and/or diuretic is increased.
Administration
Enalaprilat injection should be administered as a slow intravenous infusion, as indicated above. It may be administered as provided or diluted with up to 50 mL of a compatible diluent.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to use whenever solution and container permit.
Compatibility and Stability
Enalaprilat injection as supplied and mixed with the following intravenous diluents has been found to maintain full activity for 24 hours at room temperature:
5 percent Dextrose Injection
0.9 percent Sodium Chloride Injection
0.9 percent Sodium Chloride Injection in 5 percent Dextrose
5 percent Dextrose in Lactated Ringer's Injection
ISOLYTE ••• E ( ••• Registered trademark of B. Braun)
CONTRAINDICATIONS
Enalaprilat injection is contraindicated in patients who are hypersensitive to any component of this product and in patients with a history of angioedema related to previous treatment with an angiotensin-converting enzyme inhibitor and in patients with hereditary or idiopathic angioedema.
ADVERSE REACTIONS
Enalaprilat has been found to be generally well tolerated in controlled clinical trials involving 349 patients (168 with hypertension, 153 with congestive heart failure and 28 with coronary artery disease). The most frequent clinically significant adverse experience was hypotension (3.4 percent), occurring in eight patients (5.2 percent) with congestive heart failure, three (1.8 percent) with hypertension and one with coronary artery disease. Other adverse experiences occurring in greater than one percent of patients were: headache (2.9 percent) and nausea (1.1 percent).
Adverse experiences occurring in 0.5 to 1 percent of patients in controlled clinical trials included: myocardial infarction, fatigue, dizziness, fever, rash and constipation.
Angioedema : Angioedema has been reported in patients receiving enalaprilat, with an incidence higher in black than in non-black patients. Angioedema associated with laryngeal edema may be fatal. If angioedema of the face, extremities, lips, tongue, glottis and/or larynx occurs, treatment with enalaprilat should be discontinued and appropriate therapy instituted immediately (see WARNINGS ).
Cough: See PRECAUTIONS, Cough .
Enalapril Maleate
Since enalapril is converted to enalaprilat, those adverse experiences associated with enalapril might also be expected to occur with enalaprilat injection.
The following adverse experiences have been reported with enalapril and, within each category, are listed in order of decreasing severity.
Body as a Whole : Syncope, orthostatic effects, anaphylactoid reactions (see WARNINGS, Anaphylactoid reactions during membrane exposure ), chest pain, abdominal pain, asthenia.
Cardiovascular : Cardiac arrest; myocardial infarction or cerebrovascular accident, possibly secondary to excessive hypotension in high risk patients (see WARNINGS,Hypotension ); pulmonary embolism and infarction; pulmonary edema; rhythm disturbances including atrial tachycardia and bradycardia; atrial fibrillation; orthostatic hypotension; angina pectoris; palpitation, Raynaud's phenomenon.
Digestive : Ileus, pancreatitis, hepatic failure, hepatitis (hepatocellular [proven on rechallenge] or cholestatic jaundice) (see WARNINGS, Hepatic Failure ), melena, diarrhea, vomiting, dyspepsia, anorexia, glossitis, stomatitis, dry mouth.
Hematologic : Rare cases of neutropenia, thrombocytopenia and bone marrow depression.
Musculoskeletal : Muscle cramps.
Nervous/Psychiatric : Depression, vertigo, confusion, ataxia, somnolence, insomnia, nervousness, peripheral neuropathy (e.g., paresthesia, dysesthesia), dream abnormality.
Respiratory: Bronchospasm, dyspnea, pneumonia, bronchitis, cough, rhinorrhea, sore throat and hoarseness, asthma, upper respiratory infection, pulmonary infiltrates, eosinophilic pneumonitis.
Skin : Exfoliative dermatitis, toxic epidermal necrolysis, Stevens-Johnson syndrome, pemphigus, herpes zoster, erythema multiforme, urticaria, pruritus, alopecia, flushing, diaphoresis, photosensitivity.
Special Senses : Blurred vision, taste alteration, anosmia, tinnitus, conjunctivitis, dry eyes, tearing.
Urogenital : Renal failure, oliguria, renal dysfunction (see PRECAUTIONS and DOSAGE AND ADMINISTRATION ), urinary tract infection, flank pain, gynecomastia, impotence.
Miscellaneous : A symptom complex has been reported which may include some or all of the following: a positive ANA, an elevated erythrocyte sedimentation rate, arthralgia/arthritis, myalgia/myositis, fever, serositis, vasculitis, leukocytosis, eosinophilia, photosensitivity, rash and other dermatologic manifestations.
Hypotension : Combining the results of clinical trials in patients with hypertension or congestive heart failure, hypotension (including postural hypotension, and other orthostatic effects) was reported in 2.3 percent of patients following the initial dose of enalapril or during extended therapy. In the hypertensive patients, hypotension occurred in 0.9 percent and syncope occurred in 0.5 percent of patients. Hypotension or syncope was a cause for discontinuation of therapy in 0.1 percent of hypertensive patients (see WARNINGS ).
Fetal/Neonatal Morbidity and Mortality : See WARNINGS, Fetal/Neonatal Morbidity and Mortality .
Clinical Laboratory Test Findings
Serum Electrolytes : Hyperkalemia (see PRECAUTIONS ), hyponatremia.
Creatinine, Blood Urea Nitrogen: In controlled clinical trials minor increases in blood urea nitrogen and serum creatinine, reversible upon discontinuation of therapy, were observed in about 0.2 percent of patients with essential hypertension treated with enalapril alone. Increases are more likely to occur in patients receiving concomitant diuretics or in patients with renal artery stenosis (see PRECAUTIONS ).
Hematology : Small decreases in hemoglobin and hematocrit (mean decreases of approximately 0.3 g percent and 1 vol percent, respectively) occur frequently in hypertensive patients treated with enalapril but are rarely of clinical importance unless another cause of anemia coexists. In clinical trials, less than 0.1 percent of patients discontinued therapy due to anemia. Hemolytic anemia, including cases of hemolysis in patients with G-6-PD deficiency, has been reported; a causal relationship to enalapril cannot be excluded.
Liver Function Tests : Elevations of liver enzymes and/or serum bilirubin have occurred (see WARNINGS, Hepatic Failure ).
Drug Interactions
Hypotension-Patients on Diuretic Therapy : Patients on diuretics and especially those in whom diuretic therapy was recently instituted, may occasionally experience an excessive reduction of blood pressure after initiation of therapy with enalaprilat. The possibility of hypotensive effects with enalaprilat can be minimized by administration of an intravenous infusion of normal saline, discontinuing the diuretic or increasing the salt intake prior to initiation of treatment with enalaprilat. If it is necessary to continue the diuretic, provide close medical supervision for at least one hour after the initial dose of enalaprilat (see WARNINGS ).
Agents Causing Renin Release : The antihypertensive effect of enalaprilat injection appears to be augmented by antihypertensive agents that cause renin release (e.g., diuretics).
Non-Steroidal Anti-Inflammatory Agents : In some patients with compromised renal function who are being treated with non-steroidal anti-inflammatory drugs, the coadministration of enalapril may result in a further deterioration of renal function. These effects are usually reversible.
In a clinical pharmacology study, indomethacin or sulindac was administered to hypertensive patients receiving enalapril maleate. In this study there was no evidence of a blunting of the antihypertensive action of enalapril maleate. However, reports suggest that NSAIDs may diminish the antihypertensive effect of ACE inhibitors. This interaction should be given consideration in patients taking NSAIDs concomitantly with ACE inhibitors.
Other Cardiovascular Agents: Enalaprilat injection has been used concomitantly with digitalis, beta adrenergic-blocking agents, methyldopa, nitrates, calcium-blocking agents, hydralazine and prazosin without evidence of clinically significant adverse interactions.
Agents Increasing Serum Potassium : Enalaprilat injection attenuates potassium loss caused by thiazide-type diuretics. Potassium-sparing diuretics (e.g., spironolactone, triamterene, or amiloride), potassium supplements, or potassium-containing salt substitutes may lead to significant increases in serum potassium. Therefore, if concomitant use of these agents is indicated because of demonstrated hypokalemia, they should be used with caution and with frequent monitoring of serum potassium.
Lithium : Lithium toxicity has been reported in patients receiving lithium concomitantly with drugs which cause elimination of sodium, including ACE inhibitors. A few cases of lithium toxicity have been reported in patients receiving concomitant enalapril and lithium and were reversible upon discontinuation of both drugs. It is recommended that serum lithium levels be monitored frequently if enalapril is administered concomitantly with lithium.
Gold : Nitritoid reactions (symptoms include facial flushing, nausea, vomiting and hypotension) have been reported rarely in patients on therapy with injectable gold (sodium aurothiomalate) and concomitant ACE inhibitor therapy.
DESCRIPTION
Enalaprilat injection, USP is a sterile aqueous solution for intravenous administration. Enalaprilat is an angiotensin-converting enzyme inhibitor. It is chemically described as (S)-1-[N-(1-carboxy-3-phenylpropyl)-L-alanyl]-L-proline dihydrate. Its molecular formula is C 18 H 24 N 2 O 5 •2H 2 O and its structural formula is:
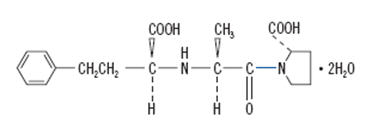
Enalaprilat, USP is a white or almost white crystalline powder with a molecular weight of 384.43. It is sparingly soluble in methanol and slightly soluble in water.
Each milliliter of enalaprilat injection, USP contains 1.25 mg enalaprilat, USP (anhydrous equivalent); sodium chloride to adjust tonicity; sodium hydroxide to adjust pH; water for injection, q.s.; with benzyl alcohol, 9 mg, added as a preservative.
CLINICAL PHARMACOLOGY
Enalaprilat, an angiotensin-converting enzyme (ACE) inhibitor when administered intravenously, is the active metabolite of the orally administered pro-drug, enalapril maleate. Enalaprilat is poorly absorbed orally.
Mechanism of Action
Intravenous enalaprilat, or oral enalapril, after hydrolysis to enalaprilat, inhibits ACE in human subjects and animals. ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. Although the latter decrease is small, it results in small increases of serum potassium. In hypertensive patients treated with enalapril alone for up to 48 weeks, mean increases in serum potassium of approximately 0.2 mEq/L were observed. In patients treated with enalapril plus a thiazide diuretic, there was essentially no change in serum potassium (see PRECAUTIONS ). Removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of enalaprilat remains to be elucidated.
While the mechanism through which enalaprilat lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, enalaprilat has anti-hypertensive activity even in patients with low-renin hypertension. In clinical studies, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to enalaprilat monotherapy than non-black patients.
Pharmacokinetics and Metabolism
Following intravenous administration of a single dose, the serum concentration profile of enalaprilat is polyexponential with a prolonged terminal phase, apparently representing a small fraction of the administered dose that has been bound to ACE. The amount bound does not increase with dose, indicating a saturable site of binding. The effective half-life for accumulation of enalaprilat, as determined from oral administration of multiple doses of enalapril maleate, is approximately 11 hours. Excretion of enalaprilat is primarily renal with more than 90 percent of an administered dose recovered in the urine as unchanged drug within 24 hours. Enalaprilat is poorly absorbed following oral administration.
The disposition of enalaprilat in patients with renal insufficiency is similar to that in patients with normal renal function until the glomerular filtration rate is 30 mL/min or less. With glomerular filtration rate ≤30 mL/min, peak and trough enalaprilat levels increase, time to peak concentration increases and time to steady state may be delayed. The effective half-life of enalaprilat is prolonged at this level of renal insufficiency (see DOSAGE AND ADMINISTRATION ). Enalaprilat is dialyzable at the rate of 62 mL/min.
Studies in dogs indicate that enalaprilat does not enter the brain, and that enalapril crosses the blood-brain barrier poorly, if at all. Multiple doses of enalapril maleate in rats do not result in accumulation in any tissues. Milk in lactating rats contains radioactivity following administration of 14 C enalapril maleate. Radioactivity was found to cross the placenta following administration of labeled drug to pregnant hamsters.
Pharmacodynamics
Enalaprilat injection results in the reduction of both supine and standing systolic and diastolic blood pressure, usually with no orthostatic component. Symptomatic postural hypotension is therefore infrequent, although it might be anticipated in volume-depleted patients (see WARNINGS ). The onset of action usually occurs within fifteen minutes of administration with the maximum effect occurring within one to four hours. The abrupt withdrawal of enalaprilat has not been associated with a rapid increase in blood pressure. The duration of hemodynamic effects appears to be dose-related. However, for the recommended dose, the duration of action in most patients is approximately six hours.
Following administration of enalapril, there is an increase in renal blood flow; glomerular filtration rate is usually unchanged. The effects appear to be similar in patients with renovascular hypertension.
In a clinical pharmacology study, indomethacin or sulindac was administered to hypertensive patients receiving enalapril maleate. In this study there was no evidence of a blunting of the antihypertensive action of enalapril maleate (see PRECAUTIONS, Drug Interactions ).
HOW SUPPLIED
Enalaprilat Injection USP, 1.25 mg/mL is a clear, colorless solution free from visible particulate matter and is available as follows:
| Enalaprilat Injection USP, 1.25 mg/mL | NDC 43598-078-58 | 10 vials per carton |
| Enalaprilat Injection USP, 2.5 mg/2 mL | NDC 43598-169-58 | 10 vials per carton |
Storage
Store at 20°C to 25°C (68°F to 77°F) [See USP Controlled Room Temperature].
To report SUSPECTED ADVERSE REACTIONS, contact Dr. Reddy’s Laboratories Inc., at 1-888-375-3784 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
Distributor:
Dr. Reddy’s Laboratories Inc.,
Princeton, NJ 08540
Made in India
Revised: 04/2023
Mechanism of Action
Intravenous enalaprilat, or oral enalapril, after hydrolysis to enalaprilat, inhibits ACE in human subjects and animals. ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. Although the latter decrease is small, it results in small increases of serum potassium. In hypertensive patients treated with enalapril alone for up to 48 weeks, mean increases in serum potassium of approximately 0.2 mEq/L were observed. In patients treated with enalapril plus a thiazide diuretic, there was essentially no change in serum potassium (see PRECAUTIONS ). Removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of enalaprilat remains to be elucidated.
While the mechanism through which enalaprilat lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, enalaprilat has anti-hypertensive activity even in patients with low-renin hypertension. In clinical studies, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to enalaprilat monotherapy than non-black patients.