Get your patient on Dipyridamole - Dipyridamole tablet, Film Coated (Dipyridamole)
Dipyridamole - Dipyridamole tablet, Film Coated prescribing information
INDICATIONS AND USAGE
Dipyridamole tablets are indicated as an adjunct to coumarin anticoagulants in the prevention of postoperative thromboembolic complications of cardiac valve replacement.
DOSAGE AND ADMINISTRATION
Adjunctive Use in Prophylaxis of Thromboembolism after Cardiac Valve Replacement. The recommended dose is 75-100 mg four times daily as an adjunct to the usual warfarin therapy. Please note that aspirin is not to be administered concomitantly with coumarin anticoagulants.
CONTRAINDICATIONS
Hypersensitivity to dipyridamole and any of the other components.
ADVERSE REACTIONS
Adverse reactions at therapeutic doses are usually minimal and transient. On long-term use of dipyridamole tablets initial side effects usually disappear. The following reactions in Table 1 were reported in two heart valve replacement trials comparing dipyridamole tablets and warfarin therapy to either warfarin alone or warfarin and placebo:
| Adverse Reaction | Dipyridamole Tablets/ Warfarin | Placebo/ Warfarin |
|---|---|---|
| Number of patients | 147 | 170 |
| Dizziness | 13.6% | 8.2% |
| Abdominal distress | 6.1% | 3.5% |
| Headache | 2.3% | 0.0% |
| Rash | 2.3% | 1.1% |
Other reactions from uncontrolled studies include diarrhea, vomiting, flushing and pruritus. In addition, angina pectoris has been reported rarely and there have been rare reports of liver dysfunction. On those uncommon occasions when adverse reactions have been persistent or intolerable, they have ceased on withdrawal of the medication.
When dipyridamole tablets were administered concomitantly with warfarin, bleeding was no greater in frequency or severity than that observed when warfarin was administered alone. In rare cases, increased bleeding during or after surgery has been observed.
In post-marketing reporting experience, there have been rare reports of hypersensitivity reactions (such as rash, urticaria, severe bronchospasm, and angioedema), larynx edema, fatigue, malaise, myalgia, arthritis, nausea, dyspepsia, paresthesia, hepatitis, thrombocytopenia, alopecia, cholelithiasis, hypotension, palpitation, and tachycardia.
Drug Interactions
No pharmacokinetic drug-drug interaction studies were conducted with dipyridamole tablets. The following information was obtained from the literature.
Adenosinergic agents (e.g., adenosine, regadenoson): Dipyridamole has been reported to increase the plasma levels and cardiovascular effects of adenosine. Adjustment of adenosine dosage may be necessary. Dipyridamole also increases the cardiovascular effects of regadenoson, an adenosine A2A-receptor agonist. The potential risk of cardiovascular side effects with intravenous adenosinergic agents may be increased during the testing period when dipyridamole is not held 48 hours prior to stress testing.
Cholinesterase Inhibitors: Dipyridamole may counteract the anticholinesterase effect of cholinesterase inhibitors, thereby potentially aggravating myasthenia gravis.
DESCRIPTION
Dipyridamole USP is a platelet inhibitor chemically described as 2,2',2'',2'''-[(4,8 Dipiperidinopyrimido[5,4- d ]pyrimidine-2,6-diyl)dinitrilo]-tetraethanol. It has the following structural formula:
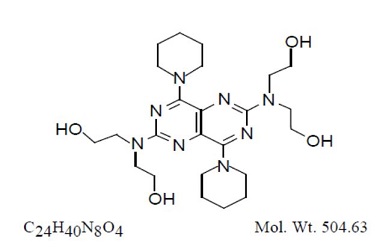
Dipyridamole is an odorless yellow crystalline powder, having a bitter taste. It is soluble in dilute acids, methanol and chloroform, and practically insoluble in water.
Dipyridamole tablets for oral administration contain:
Active Ingredient TABLETS 25 mg, 50 mg, and 75 mg : dipyridamole USP 25 mg, 50 mg and 75 mg, respectively.
Inactive Ingredients TABLETS 25 mg, 50 mg, and 75 mg : Carnauba wax, D&C yellow no. 10, FD&C yellow no. 6, hydroxypropyl cellulose, hypromellose, lactose, magnesium stearate, methylparaben, microcrystalline cellulose, polyethylene glycol, potassium sorbate, povidone, propylene glycol, propylparaben, silicon dioxide, sodium citrate, sodium starch glycolate, stearic acid, talc, titanium dioxide, and xanthan gum.
CLINICAL PHARMACOLOGY
It is believed that platelet reactivity and interaction with prosthetic cardiac valve surfaces, resulting in abnormally shortened platelet survival time, is a significant factor in thromboembolic complications occurring in connection with prosthetic heart valve replacement.
Dipyridamole tablets have been found to lengthen abnormally shortened platelet survival time in a dose-dependent manner.
In three randomized controlled clinical trials involving 854 patients who had undergone surgical placement of a prosthetic heart valve, dipyridamole tablets, in combination with warfarin, decreased the incidence of postoperative thromboembolic events by 62 to 91% compared to warfarin treatment alone. The incidence of thromboembolic events in patients receiving the combination of dipyridamole tablets and warfarin ranged from 1.2 to 1.8%. In three additional studies involving 392 patients taking dipyridamole tablets and coumarin-like anticoagulants, the incidence of thromboembolic events ranged from 2.3 to 6.9%.
In these trials, the coumarin anticoagulant was begun between 24 hours and 4 days postoperatively, and the dipyridamole tablets were begun between 24 hours and 10 days postoperatively. The length of follow-up in these trials varied from 1 to 2 years.
Dipyridamole tablets do not influence prothrombin time or activity measurements when administered with warfarin.
Mechanism of Action
Dipyridamole inhibits the uptake of adenosine into platelets, endothelial cells and erythrocytes in vitro and in vivo ; the inhibition occurs in a dose-dependent manner at therapeutic concentrations (0.5-1.9 mg/mL). This inhibition results in an increase in local concentrations of adenosine which acts on the platelet A 2 -receptor thereby stimulating platelet adenylate cyclase and increasing platelet cyclic-3',5'-adenosine monophosphate (cAMP) levels. Via this mechanism, platelet aggregation is inhibited in response to various stimuli such as platelet activating factor (PAF), collagen and adenosine diphosphate (ADP).
Dipyridamole inhibits phosphodiesterase (PDE) in various tissues. While the inhibition of cAMP-PDE is weak, therapeutic levels of dipyridamole inhibit cyclic-3',5'-guanosine monophosphate-PDE (cGMP-PDE), thereby augmenting the increase in cGMP produced by EDRF (endothelium-derived relaxing factor, now identified as nitric oxide).
Hemodynamics
In dogs intraduodenal doses of dipyridamole of 0.5 to 4.0 mg/kg produced dose-related decreases in systemic and coronary vascular resistance leading to decreases in systemic blood pressure and increases in coronary blood flow. Onset of action was in about 24 minutes and effects persisted for about 3 hours.
Similar effects were observed following intravenous dipyridamole in doses ranging from 0.025 to 2.0 mg/kg.
In man the same qualitative hemodynamic effects have been observed. However, acute intravenous administration of dipyridamole may worsen regional myocardial perfusion distal to partial occlusion of coronary arteries.
Pharmacokinetics and Metabolism
Following an oral dose of dipyridamole tablets, the average time to peak concentration is about 75 minutes. The decline in plasma concentration following a dose of dipyridamole tablets fits a two-compartment model. The alpha half-life (the initial decline following peak concentration) is approximately 40 minutes. The beta half-life (the terminal decline in plasma concentration) is approximately 10 hours. Dipyridamole is highly bound to plasma proteins. It is metabolized in the liver where it is conjugated as a glucuronide and excreted with the bile.
HOW SUPPLIED
Dipyridamole tablets, USP are available as yellow, round, biconvex, coated tablets debossed tablets of 25 mg, 50 mg and 75 mg coded “181”, ”182” and ”183”, respectively on one side and “O” on the other.
They are available in bottles of 100 tablets as indicated below:
25 mg Tablets (NDC 69584-181-10) 50 mg Tablets (NDC 69584-182-10) 75 mg Tablets (NDC 69584-183-10)
Store at 20°– 25°C (68°– 77°F) [see USP Controlled Room Temperature]. Keep out of reach of children.
Address medical inquiries to: 1-844‑508‑1455, 8:00 AM to 4.30 PM ET, Monday – Friday
Manufactured by: OXFORD PHARMACEUTICALS Birmingham, AL 35211
8200025 Rev 00 01/21
Mechanism of Action
Dipyridamole inhibits the uptake of adenosine into platelets, endothelial cells and erythrocytes in vitro and in vivo ; the inhibition occurs in a dose-dependent manner at therapeutic concentrations (0.5-1.9 mg/mL). This inhibition results in an increase in local concentrations of adenosine which acts on the platelet A 2 -receptor thereby stimulating platelet adenylate cyclase and increasing platelet cyclic-3',5'-adenosine monophosphate (cAMP) levels. Via this mechanism, platelet aggregation is inhibited in response to various stimuli such as platelet activating factor (PAF), collagen and adenosine diphosphate (ADP).
Dipyridamole inhibits phosphodiesterase (PDE) in various tissues. While the inhibition of cAMP-PDE is weak, therapeutic levels of dipyridamole inhibit cyclic-3',5'-guanosine monophosphate-PDE (cGMP-PDE), thereby augmenting the increase in cGMP produced by EDRF (endothelium-derived relaxing factor, now identified as nitric oxide).