Get your patient on Cleocin - Clindamycin Phosphate suppository (Clindamycin Phosphate)
Cleocin - Clindamycin Phosphate suppository prescribing information
INDICATIONS AND USAGE
CLEOCIN Vaginal Ovules are indicated for 3-day treatment of bacterial vaginosis in non-pregnant women. There are no adequate and well-controlled studies of CLEOCIN Vaginal Ovules in pregnant women.
NOTE: For purposes of this indication, a clinical diagnosis of bacterial vaginosis is usually defined by the presence of a homogeneous vaginal discharge that (a) has a pH of greater than 4.5, (b) emits a "fishy" amine odor when mixed with a 10% KOH solution, and (c) contains clue cells on microscopic examination. Gram's stain results consistent with a diagnosis of bacterial vaginosis include (a) markedly reduced or absent Lactobacillus morphology, (b) predominance of Gardnerella morphotype, and (c) absent or few white blood cells.
Other pathogens commonly associated with vulvovaginitis, e.g., Trichomonas vaginalis , Chlamydia trachomatis , Neisseria gonorrhoeae , Candida albicans , and herpes simplex virus, should be ruled out.
DOSAGE AND ADMINISTRATION
The recommended dose is one CLEOCIN Vaginal Ovule (containing clindamycin phosphate equivalent to 100 mg clindamycin per 2.5 g suppository) intravaginally per day, preferably at bedtime, for 3 consecutive days.
CONTRAINDICATIONS
CLEOCIN Vaginal Ovules are contraindicated in individuals with a history of hypersensitivity to clindamycin, lincomycin, or any of the components of this vaginal suppository. CLEOCIN Vaginal Ovules are also contraindicated in individuals with a history of regional enteritis, ulcerative colitis, or a history of "antibiotic-associated" colitis.
ADVERSE REACTIONS
Clinical Trials
In clinical trials, 3 (0.5%) of 589 nonpregnant women who received treatment with CLEOCIN Vaginal Ovules discontinued therapy due to drug-related adverse events. Adverse events judged to have a reasonable possibility of having been caused by clindamycin phosphate vaginal suppositories were reported for 10.5% of patients. Events reported by 1% or more of patients receiving CLEOCIN Vaginal Ovules were as follows:
Urogenital system: Vulvovaginal disorder (3.4%), vaginal pain (1.9%), and vaginal moniliasis (1.5%).
Body as a whole: Fungal infection (1.0%).
Other events reported by <1% of patients included:
Urogenital system: Menstrual disorder, dysuria, pyelonephritis, vaginal discharge, and vaginitis/vaginal infection.
Body as a whole: Abdominal cramps, localized abdominal pain, fever, flank pain, generalized pain, headache, localized edema, and moniliasis.
Digestive system: Diarrhea, nausea, and vomiting.
Skin: Nonapplication-site pruritis, rash, application-site pain, and application-site pruritis.
Other clindamycin formulations
The overall systemic exposure to clindamycin from CLEOCIN Vaginal Ovules is substantially lower than the systemic exposure from therapeutic doses of oral clindamycin hydrochloride (two-fold to 20-fold lower) or parenteral clindamycin phosphate (40-fold to 50-fold lower). (See CLINICAL PHARMACOLOGY .) Although these lower levels of exposure are less likely to produce the common reactions seen with oral or parenteral clindamycin, the possibility of these and other reactions cannot be excluded.
The following adverse reactions and altered laboratory tests have been reported with the oral or parenteral use of clindamycin and may also occur following administration of CLEOCIN Vaginal Ovules:
Infections and Infestations: Clostridioides difficile colitis
Gastrointestinal: Abdominal pain, esophagitis, nausea, vomiting, diarrhea, and pseudomembranous colitis. (See WARNINGS .)
Hematopoietic: Transient neutropenia (leukopenia), eosinophilia, agranulocytosis, and thrombocytopenia have been reported. No direct etiologic relationship to concurrent clindamycin therapy could be made in any of these reports.
Hypersensitivity Reactions: Maculopapular rash and urticaria have been observed during drug therapy. Generalized mild to moderate morbilliform-like skin rashes are the most frequently reported of all adverse reactions. Cases of Acute Generalized Exanthematous Pustulosis (AGEP), erythema multiforme, some resembling Stevens-Johnson syndrome, have been associated with clindamycin. A few cases of anaphylactoid reactions have been reported. If a hypersensitivity reaction occurs, the drug should be discontinued.
Liver: Jaundice and abnormalities in liver function tests have been observed during clindamycin therapy.
Musculoskeletal: Cases of polyarthritis have been reported.
Renal: Acute kidney injury
Immune System: Drug reaction with eosinophilia and systemic symptoms (DRESS) cases have been reported.
There have been reports of pseudomembranous colitis following the administration of clindamycin vaginal cream.
Drug Interactions
Systemic clindamycin has been shown to have neuromuscular blocking properties that may enhance the action of other neuromuscular blocking agents. Therefore, it should be used with caution in patients receiving such agents.
DESCRIPTION
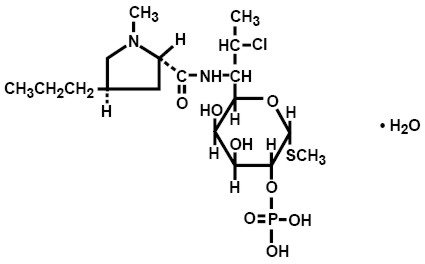
Clindamycin phosphate is a water-soluble ester of the semisynthetic antibiotic produced by a 7(S)-chloro-substitution of the 7(R)-hydroxyl group of the parent antibiotic lincomycin. The chemical name for clindamycin phosphate is methyl 7-chloro-6,7,8-trideoxy-6-(1-methyl- trans -4-propyl-L-2-pyrrolidinecarboxamido)-1-thio-L- threo -α-D- galacto -octopyranoside 2-(dihydrogen phosphate). The monohydrate form has a molecular weight of 522.98, and the molecular formula is C 18 H 34 ClN 2 O 8 PS•H 2 O. The structural formula is represented below:
CLEOCIN Vaginal Ovules are semisolid, white to off-white suppositories for intravaginal administration. Each 2.5 g suppository contains clindamycin phosphate equivalent to 100 mg clindamycin in a base consisting of a mixture of glycerides of saturated fatty acids.
CLINICAL PHARMACOLOGY
Mechanism of Action
Clindamycin is an antibacterial drug (See MICROBIOLOGY ).
Pharmacokinetics
Systemic absorption of clindamycin was estimated following a once-a-day intravaginal dose of one clindamycin phosphate vaginal suppository (equivalent to 100 mg clindamycin) administered to 11 healthy female volunteers for 3 days. Approximately 30% (range 6% to 70%) of the administered dose was absorbed systemically on day 3 of dosing based on area under the concentration-time curve (AUC). Systemic absorption was estimated using a subtherapeutic 100 mg intravenous dose of clindamycin phosphate as a comparator in the same volunteers. The mean AUC following day 3 of dosing with the suppository was 3.2 µg hr/mL (range 0.42 to 11 µg hr/mL). The C max observed on day 3 of dosing with the suppository averaged 0.27 µg/mL (range 0.03 to 0.67 µg/mL) and was observed about 5 hours after dosing (range 1 to 10 hours). In contrast, the AUC and C max after the single intravenous dose averaged 11 µg hr/mL (range 5.1 to 26 µg hr/mL) and 3.7 µg/mL (range 2.4 to 5.0 µg/mL), respectively. The mean apparent elimination half-life after dosing with the suppository was 11 hours (range 4 to 35 hours) and is considered to be limited by the absorption rate.
The results from this study showed that systemic exposure to clindamycin (based on AUC) from the suppository was, on average, three-fold lower than that from a single subtherapeutic 100 mg intravenous dose of clindamycin. In addition, the recommended daily and total doses of intravaginal clindamycin suppository are far lower than those typically administered in oral or parenteral clindamycin therapy (100 mg of clindamycin per day for 3 days equivalent to about 30 mg absorbed per day from the ovule relative to 600 to 2700 mg/day for up to 10 days or more, orally or parenterally). The overall systemic exposure to clindamycin from Cleocin Vaginal Ovules is substantially lower than the systemic exposure from therapeutic doses of oral clindamycin hydrochloride (two-fold to 20-fold lower) or parenteral clindamycin phosphate (40-fold to 50-fold lower).
Clinical Trials
In clinical trials, 3 (0.5%) of 589 nonpregnant women who received treatment with CLEOCIN Vaginal Ovules discontinued therapy due to drug-related adverse events. Adverse events judged to have a reasonable possibility of having been caused by clindamycin phosphate vaginal suppositories were reported for 10.5% of patients. Events reported by 1% or more of patients receiving CLEOCIN Vaginal Ovules were as follows:
Urogenital system: Vulvovaginal disorder (3.4%), vaginal pain (1.9%), and vaginal moniliasis (1.5%).
Body as a whole: Fungal infection (1.0%).
Other events reported by <1% of patients included:
Urogenital system: Menstrual disorder, dysuria, pyelonephritis, vaginal discharge, and vaginitis/vaginal infection.
Body as a whole: Abdominal cramps, localized abdominal pain, fever, flank pain, generalized pain, headache, localized edema, and moniliasis.
Digestive system: Diarrhea, nausea, and vomiting.
Skin: Nonapplication-site pruritis, rash, application-site pain, and application-site pruritis.
HOW SUPPLIED
CLEOCIN Vaginal Ovule is supplied as follows:
Carton of three suppositories without the applicator | NDC 0009-7667-05 |
Important Information: Store at 25°C (77°F); excursions permitted to 15 – 30°C (59 – 86°F) [see USP Controlled Room Temperature].
Caution: Avoid heat over 30°C (86°F). Avoid high humidity. See end of carton for the lot number and expiration date.