Get your patient on Betaxolol Hydrochloride - Betaxolol Hydrochloride tablet, Coated (Betaxolol Hydrochloride)
Betaxolol Hydrochloride - Betaxolol Hydrochloride tablet, Coated prescribing information
INDICATIONS AND USAGE:
Betaxolol tablets, USP is indicated in the management of hypertension. It may be used alone or concomitantly with other antihypertensive agents, particularly thiazide-type diuretics.
DOSAGE AND ADMINISTRATION:
The initial dose of betaxolol tablets, USP in hypertension is ordinarily 10 mg once daily either alone or added to diuretic therapy. The full antihypertensive effect is usually seen within 7 to 14 days. If the desired response is not achieved the dose can be doubled after 7 to 14 days. Increasing the dose beyond 20 mg has not been shown to produce a statistically significant additional antihypertensive effect; but the 40-mg dose has been studied and is well tolerated. An increased effect (reduction) on heart rate should be anticipated with increasing dosage. If monotherapy with betaxolol tablets, USP does not produce the desired response, the addition of a diuretic agent or other antihypertensive should be considered (see PRECAUTIONS, Drug Interactions ).
Dosage Adjustments For Specific Patients:
Patients with renal failure:
In patients with renal impairment, clearance of betaxolol declines with decreasing renal function.
In patients with severe renal impairment and those undergoing dialysis, the initial dose of betaxolol tablets, USP is 5 mg once daily. If the desired response is not achieved, dosage may be increased by 5 mg/day increments every 2 weeks to a maximum dose of 20 mg/day.
Patients with hepatic disease:
Patients with hepatic disease do not have significantly altered clearance. Dosage adjustments are not routinely needed.
Elderly patients:
Consideration should be given to reduction in the starting dose to 5 mg in elderly patients. These patients are especially prone to beta-blocker-induced bradycardia, which appears to be dose related and sometimes responds to reductions in dose.
Cessation of therapy:
If withdrawal of betaxolol tablets, USP therapy is planned, it should be achieved gradually over a period of about 2 weeks. Patients should be carefully observed and advised to limit physical activity to a minimum.
CONTRAINDICATIONS:
Betaxolol tablets, USP is contraindicated in patients with known hypersensitivity to the drug.
Betaxolol tablets, USP is contraindicated in patients with sinus bradycardia, heart block greater than first degree, cardiogenic shock, and overt cardiac failure (see Warnings ).
ADVERSE REACTIONS:
Most adverse reactions have been mild and transient and are typical of beta-adrenergic blocking agents, e.g., bradycardia, fatigue, dyspnea, and lethargy. Withdrawal of therapy in U.S. and European controlled clinical trials has been necessary in about 3.5% of patients, principally because of bradycardia, fatigue, dizziness, headache, and impotence. Frequency estimates of adverse events were derived from controlled studies in which adverse reactions were volunteered and elicited in U.S. studies and volunteered and/or elicited in European studies.
In the U.S., the placebo-controlled hypertension studies lasted for 4 weeks, while the active-controlled hypertension studies has a 22- to 24- week double-blind phase. The following doses were studied: Betaxolol tablets, USP-5, 10, 20, and 40 mg once daily; atenolol-25, 50, and 100 mg once daily; and propranolol-40, 80, and 160 mg b.i.d.
Betaxolol tablets, USP, like other beta-blockers, has been associated with the development of antinuclear antibodies (ANA) (e.g. lupus erythematosus). In controlled clinical studies, conversion of ANA from negative to positive occurred in 5.3% of the patients treated with betaxolol tablets, USP, 6.3% of the patients treated with atenolol, 4.9% of the patients treated with propranolol, and 3.2% of the patients treated with placebo.
Betaxolol adverse events reported with a 2% or greater frequency, and selected events with lower frequency, in U.S. controlled studies are:
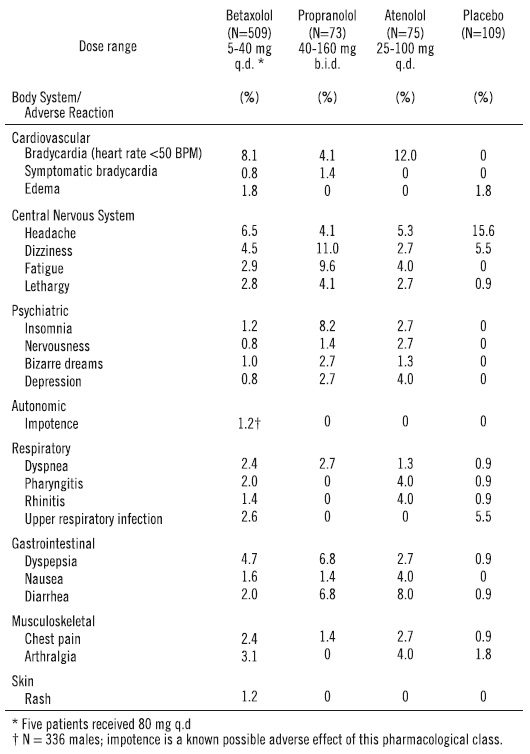
Of the above adverse reactions associated with the use of betaxolol, only bradycardia was clearly dose related, but there was a suggestion of dose relatedness for fatigue, lethargy, and dyspepsia.
In Europe, the placebo-controlled study lasted for 4 weeks, while the comparative studies had a 4- to 52-week double-blind phase. The following doses were studied: Betaxolol 20 and 40 mg once daily and atenolol 100 mg once daily.
From European controlled hypertension clinical trials, the following adverse events reported by 2% or more patients and selected events with lower frequency are presented:
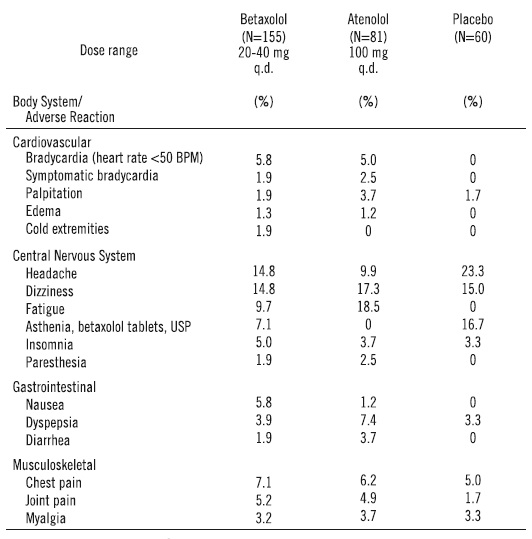
The only adverse event whose frequency clearly rose with increasing dose was bradycardia. Elderly patients were especially susceptible to bradycardia, which in some cases responded to dose-reduction (see Precautions ).
The following selected (potentially important) adverse events have been reported at an incidence of less than 2% in U.S. controlled hypertension and open, long-term clinical studies, European controlled clinical trials, or in marketing experience. It is not known whether a causal relationship exists between betaxolol tablets, USP and these events; they are listed to alert the physician to a possible relationship:
Autonomic: flushing, salivation, sweating.
Body as a whole: allergy, fever, malaise, pain, rigors.
Cardiovascular: angina pectoris, arrhythmia, atrioventricular block, heart failure, hypertension, hypotension, myocardial infarction, thrombosis, syncope.
Central and peripheral nervous system: ataxia, neuralgia, neuropathy, numbness, speech disorder, stupor, tremor, twitching.
Gastrointestinal: anorexia, constipation, dry mouth, increased appetite, mouth ulceration, rectal disorders, vomiting, dysphagia.
Hearing and Vestibular: earache, labyrinth disorders, tinnitus, deafness.
Hematologic: anemia, leucocytosis, lymphadenopathy, purpura, thrombocytopenia.
Liver and biliary: increased AST, increased ALT.
Metabolic and nutritional: acidosis, diabetes, hypercholesterolemia, hyperglycemia, hyperkalemia, hyperlipemia, hyperuricemia, hypokalemia, weight gain, weight loss, thirst, increased LDH.
Musculoskeletal: arthropathy, neck pain, muscle cramps, tendonitis.
Psychiatric: abnormal thinking, amnesia, impaired concentration, confusion, emotional lability, hallucinations, decreased libido.
Reproductive disorders: Female: breast pain, breast fibroadenosis, menstrual disorder; Male: Peyronie’s disease, prostatitis.
Respiratory: bronchitis, bronchospasm, cough, epistaxis, flu, pneumonia, sinusitis.
Skin: alopecia, eczema, erythematous rash, hypertrichosis, pruritus, skin disorders.
Special senses: abnormal taste, taste loss.
Urinary system: cystitis, dysuria, micturition disorder, oliguria, proteinuria, abnormal renal function, renal pain.
Vascular: cerebrovascular disorder, intermittent claudication, leg cramps, peripheral ischemia, thrombophlebitis.
Vision: abnormal lacrimation, abnormal vision, blepharitis, ocular hemorrhage, conjunctivitis, dry eyes, iritis, cataract, scotoma.
Potential Adverse Effects: Although not reported in clinical studies with betaxolol tablets, USP, a variety of adverse effects have been reported with other beta-adrenergic blocking agents and may be considered potential adverse effects of betaxolol tablets, USP:
Central nervous system: Reversible mental depression progressing to catatonia, an acute reversible syndrome characterized by disorientation for time and place, short-term memory loss, emotional lability with slightly clouded sensorium, and decreased performance on neuropsychometric tests.
Allergic: Fever combined with aching and sore throat, laryngospasm, respiratory distress.
Hematologic: Agranulocytosis, thrombocytopenic purpura, and nonthrombocytopenic purpura.
Gastrointestinal: Mesenteric arterial thrombosis, ischemic colitis.
Miscellaneous: Raynaud’s phenomena. There have been reports of skin rashes and/or dry eyes associated with the use of beta-adrenergic blocking drugs. The reported incidence is small, and in most cases, the symptoms have cleared when treatment was withdrawn. Discontinuation of the drug should be considered if any such reaction is not otherwise explicable. Patients should be closely monitored following cessation of therapy.
The oculomucocutaneous syndrome associated with the beta-blocker practolol has not been reported with betaxolol tablets, USP during investigational use and extensive foreign experience. However, dry eyes have been reported.
DESCRIPTION:
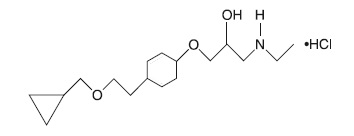
Betaxolol hydrochloride is a ß 1 -selective (cardioselective) adrenergic receptor blocking agent available as 10-mg and 20-mg tablets for oral administration. Betaxolol hydrochloride is chemically described as 2-propanol, 1- [4-[2-(cyclopropylmethoxy) ethyl] phenoxy]-3-[(1-methylethyl) amino]-, hydrochloride, (±)-. It has the following chemical structure:
Each tablet for oral administration contains 10 mg or 20 mg of betaxolol hydrochloride equivalent to 8.94 mg or 17.88 mg of betaxolol respectively. In addition, each tablet contains the following inactive ingredients, hypromellose, anhydrous lactose, microcrystalline cellulose, polyethylene glycol, polysorbate 80, pregelatinized starch, sodium starch glycolate, stearic acid and titanium dioxide.
Betaxolol hydrochloride is a water-soluble white crystalline powder with a molecular formula of C 18 H 29 NO 3 •HCl and a molecular weight of 343.9. It is freely soluble in water, ethanol, chloroform, and methanol, and has a pKa of 9.4.
CLINICAL PHARMACOLOGY:
Betaxolol is a ß 1 -selective (cardioselective) adrenergic receptor blocking agent that has weak membrane-stabilizing activity and no intrinsic sympathomimetic (partial agonist) activity. The preferential effect on ß 1 receptors is not absolute, however, and some inhibitory effects on ß 2 receptors (found chiefly in the bronchial and vascular musculature) can be expected at higher doses.
Pharmacokinetics and Metabolism: In man, absorption of an oral dose is complete. There is a small and consistent first-pass effect resulting in an absolute bioavailability of 89% ± 5% that is unaffected by the concomitant ingestion of food or alcohol. Mean peak blood concentrations of 21.6 ng/ml (range 16.3 to 27.9 ng/ml) are reached between 1.5 and 6 (mean about 3) hours after a single oral dose, in healthy volunteers, of 10 mg of betaxolol. Peak concentrations for 20-mg and 40-mg doses are 2 and 4 times that of a 10-mg dose and have been shown to be linear over the dose range of 5 to 40 mg. The peak to trough ratio of plasma concentrations over 24 hours is 2.7. The mean elimination half-life in various studies in normal volunteers ranged from about 14 to 22 hours after single oral doses and is similar in chronic dosing. Steady state plasma concentrations are attained after 5 to 7 days with once-daily dosing in persons with normal renal function.
Betaxolol is approximately 50% bound to plasma proteins. It is eliminated primarily by liver metabolism and secondarily by renal excretion. Following oral administration, greater than 80% of a dose is recovered in the urine as betaxolol and its metabolites. Approximately 15% of the dose administered is excreted as unchanged drug, the remainder being metabolites whose contribution to the clinical effect is negligible.
Steady state studies in normal volunteers and hypertensive patients found no important differences in kinetics. In patients with hepatic disease, elimination half-life was prolonged by about 33%, but clearance was unchanged, leading to little change in AUC. Dosage reductions have not routinely been necessary in these patients. In patients with chronic renal failure undergoing dialysis, mean elimination half-life was approximately doubled, as was AUC, indicating the need for a lower initial dosage (5 mg) in these patients. The clearance of betaxolol by hemodialysis was 0.015 L/h/kg and by peritoneal dialysis, 0.010 L/h/kg. In one study (n=8), patients with stable renal failure, not on dialysis, with mean creatinine clearance of 27 ml/min showed slight increases in elimination half-life and AUC, but no change in C max . In a second study of 30 hypertensive patients with mild to severe renal impairment, there was a reduction in clearance of betaxolol with increasing degrees of renal insufficiency. Inulin clearance (mL/min/1.73 m 2 ) ranged from 70 to 107 in 7 patients with mild impairment, 41 to 69 in 14 patients with moderate impairment, and 8 to 37 in 9 patients with severe impairment. Clearance following oral dosing was reduced significantly in patients with moderate and severe renal impairment (26% and 35%, respectively) when compared with those with mildly impaired renal function. In the severely impaired group, the mean C max and the mean elimination half-life tended to increase (28% and 24%, respectively) when compared with the mildly impaired group. A starting dose of 5 mg is recommended in patients with severe renal impairment. (See Dosage and Administration .)
Studies in elderly patients (n=10) gave inconsistent results but suggest some impairment of elimination, with one small study (n=4) finding a mean half-life of 30 hours. A starting dose of 5 mg is suggested in older patients.
Pharmacodynamics: Clinical pharmacology studies have demonstrated the beta-adrenergic receptor blocking activity of betaxolol by (1) reduction in resting and exercise heart rate, cardiac output, and cardiac work load, (2) reduction of systolic and diastolic blood pressure at rest and during exercise, (3) inhibition of isoproterenol-induced tachycardia, and (4) reduction of reflex orthostatic tachycardia.
The ß 1 -selectivity of betaxolol in man was shown in three ways: (1) In normal subjects, 10 and 40 mg oral doses of betaxolol tablets, USP, which reduced resting heart rate at least as much as 40 mg of propranolol, produced less inhibition of isoproterenol-induced increases in forearm blood flow and finger tremor than propranolol. In this study, 10 mg of betaxolol tablets, USP was at least comparable to 50 mg of atenolol. Both doses of betaxolol tablets, USP, and the one dose of atenolol, however, had more effect on the isoproterenol-induced changes than placebo (indicating some ß 2 effect at clinical doses) and the higher dose of betaxolol tablets, USP was more inhibitory than the lower. (2) In normal subjects, single intravenous doses of betaxolol and propranolol, which produced equal effects on exercise-induced tachycardia, had differing effects on insulin-induced hypoglycemia, with propranolol, but not betaxolol, prolonging the hypoglycemia compared with placebo. Neither drug affected the maximum extent of the hypoglycemic response. (3) In a single-blind crossover study in asthmatics (n=10), intravenous infusion over 30 minutes of low doses of betaxolol (1.5 mg) and propranolol (2 mg) had similar effects on resting heart rate but had differing effects on FEV 1 and forced vital capacity, with propranolol causing statistically significant (10% to 20%) reductions from baseline in mean values for both parameters while betaxolol had no effect on mean values. While blood levels were not measured, the dose of betaxolol used in this study would be expected to produce blood concentrations, at the time of the pulmonary function studies, considerably lower than those achieved during antihypertensive therapy with recommended doses of betaxolol. In a randomized double-blind, placebo-controlled crossover (4X4 Latin Square) study in 10 asthmatics, betaxolol (about 5 or 10 mg IV) had little effect on isoproterenol-induced increases in FEV 1 ; in contrast, propranolol (about 7 mg IV) inhibited the response.
Consistent with the negative chronotropic effect, due to beta-blockade of the SA node, and lack of intrinsic sympathomimetic activity, betaxolol increases sinus cycle length and sinus node recovery time. Conduction in the AV node is also prolonged.
Significant reductions in blood pressure and heart rate were observed 24 hours after dosing in double-blind, placebo-controlled trials with doses of 5 to 40 mg administered once daily. The antihypertensive response to betaxolol tablets, USP was similar at peak blood levels (3 to 4 hours) and at trough (24 hours). In a large randomized, parallel dose-response study of 5, 10, and 20 mg, the antihypertensive effects of the 5 mg dose were roughly half of the effects of the 20 mg dose (after adjustment for placebo effects) and the 10 mg dose gave more than 80% of the antihypertensive response to the 20 mg dose. The effect of increasing the dose from 10 mg to 20 mg was thus small. In this study, while the antihypertensive response to betaxolol tablets, USP showed a dose-response relationship, the heart rate response (reduction in HR) was not dose related. In other trials, there was little evidence of a greater antihypertensive response to 40 mg than to 20 mg. The maximum effect of each dose was achieved within 1 or 2 weeks. In comparative trials against propranolol, atenolol, and chlorthalidone, betaxolol tablets, USP appeared to be at least as effective as the comparative agent.
Betaxolol tablets, USP has been studied in combination with thiazide-type diuretics and the blood pressure effects of the combination appear additive. Betaxolol tablets, USP has also been used concurrently with methyldopa, hydralazine, and prazosin.
The mechanism of the antihypertensive effects of beta-adrenergic receptor blocking agents has not been established. Several possible mechanisms have been proposed, however, including: (1) competitive antagonism established. Several possible mechanisms have been proposed, however, including: (1) competitive antagonism of catecholamines at peripheral (especially cardiac) adrenergic-neuronal sites, leading to decreased cardiac output, (2) a central effect leading to reduced sympathetic outflow to the periphery, and (3) suppression of rennin activity.
The results from long-term studies have not shown any diminution of the antihypertensive effect of betaxolol tablets, USP with prolonged use.
HOW SUPPLIED:
Betaxolol Tablets, USP are available as follows:
Betaxolol Tablets, USP 10 mg: (Each tablet contains 10 mg betaxolol HCl equivalent to 8.94 mg betaxolol) are as white, round, film-coated biconvex tablets, debossed "k" above bisect "13" on one side and plain on the other.
Bottles of 100, NDC 10702-013-01
Betaxolol Tablets, USP 20 mg: (Each tablet contains 20 mg betaxolol HCl equivalent to 17.88 mg betaxolol) are as white, round, film-coated biconvex tablets, debossed "K" above "14" on one side and plain on the other.
Bottles of 100, NDC 10702-014-01
Store at 20° to 25°C (68° to 77°F) with excursions permitted between 15° to 30°C (59° to 86°F) [See USP Controlled Room Temperature].
Dispense in a tight container as defined in the USP, with a child-resistant closure (as required).
Manufactured by:
KVK-TECH, INC.
110 Terry Drive
Newtown, PA 18940
![]()
ID # 006037/09 04/2020
Manufacturer’s Code: 10702