Get your patient on Acyclovir - Acyclovir injection, Solution (Acyclovir)
Acyclovir - Acyclovir injection, Solution prescribing information
INDICATIONS AND USAGE
Herpes Simplex Infections in Immunocompromised Patients
Acyclovir Sodium Injection is indicated for the treatment of initial and recurrent mucosal and cutaneous herpes simplex (HSV-1 and HSV-2) in immunocompromised patients.
Initial Episodes of Herpes Genitalis
Acyclovir Sodium Injection is indicated for the treatment of severe initial clinical episodes of herpes genitalis in immunocompetent patients.
Herpes Simplex Encephalitis
Acyclovir Sodium Injection is indicated for the treatment of herpes simplex encephalitis.
Neonatal Herpes Simplex Virus Infection
Acyclovir Sodium Injection is indicated for the treatment of neonates and infants with herpes simplex infections.
Varicella-Zoster Infections in Immunocompromised Patients
Acyclovir Sodium Injection is indicated for the treatment of varicella-zoster (shingles) infections in immunocompromised patients.
DOSAGE AND ADMINISTRATION
CAUTION - RAPID OR BOLUS INTRAVENOUS INJECTION MUST BE AVOIDED (see WARNINGS and PRECAUTIONS).
INTRAMUSCULAR OR SUBCUTANEOUS INJECTION MUST BE AVOIDED (see WARNINGS).
Therapy should be initiated as early as possible following onset of signs and symptoms of herpes infections. A maximum dose equivalent to 20 mg/kg every 8 hours should not be exceeded for any patient.
Dosage
1. Herpes Simplex Infections: Mucosal and Cutaneous Herpes Simplex (HSV-1 and HSV-2) Infections in Immunocompromised Patients:
- Adults and Adolescents (Aged 12 years and older): 5 mg/kg infused at a constant rate over 1 hour, every 8 hours for 7 days.
- Pediatrics (Aged 3 months to 12 years): 10 mg/kg infused at a constant rate over 1 hour, every 8 hours for 7 days.
2. Severe Initial Clinical Episodes of Herpes Genitalis:
- Adults and Adolescents (Aged 12 years and older ): 5 mg/kg infused at a constant rate over 1 hour, every 8 hours for 5 days.
3. Herpes Simplex Encephalitis:
- Adults and Adolescents (Aged 12 years and older): 10 mg/kg infused at a constant rate over 1 hour, every 8 hours for 10 days.
- Pediatrics (Aged 3 months to 12 years): 20 mg/kg infused at a constant rate over 1 hour, every 8 hours for 10 days .
4. Neonatal Herpes Simplex Virus Infections:
- PMA of at Least 34 Weeks : 20 mg/kg infused at a constant rate over 1 hour, every 8 hours for 21 days.
- PMA of Less than 34 Weeks : 20 mg/kg infused at a constant rate over 1 hour, every 12 hours for 21 days.
In neonates with ongoing medical conditions affecting their renal function beyond the effect of prematurity, the doses recommended should be used with caution.
5. Varicella Zoster Infections: Zoster in Immunocompromised Patients:
- Adults and Adolescents (Aged 12 years and older): 10 mg/kg infused at a constant rate over 1 hour, every 8 hours for 7 days.
- Pediatrics (Younger than 12 years): 20 mg/kg infused at a constant rate over 1 hour, every 8 hours for 7 days.
- Obese Patients: Obese patients should be dosed at the recommended adult dose using Ideal Body Weight.
6. Patients with Acute or Chronic Renal Impairment (Older than 3 Months): Refer to DOSAGE AND ADMINISTRATION section for recommended doses and adjust the dosing interval as indicated in Table 6.
| Creatinine Clearance (mL/min/1.73 m 2 ) | Percent of Recommended Dose | Dosing Interval (hours) |
| > 50 | 100% | 8 |
| >25 to 50 | 100% | 12 |
| >10 to 25 | 100% | 24 |
| ≤ 10 | 50% | 24 |
Hemodialysis
For patients who require dialysis, the mean plasma half-life of acyclovir during hemodialysis is approximately 5 hours. This results in a 60% decrease in plasma concentrations following a 6-hour dialysis period. Therefore, the patient's dosing schedule should be adjusted so that an additional dose is administered after each dialysis.
Peritoneal Dialysis
No supplemental dose appears to be necessary after adjustment of the dosing interval.
Administration
The calculated dose should then be removed and added to any appropriate intravenous solution at a volume selected for administration during each 1 hour infusion. Infusion concentrations of approximately 7 mg/mL or lower are recommended. In clinical studies, the average 70 kg adult received between 60 and 150 mL of fluid per dose. Higher concentrations (e.g., 10 mg/mL) may produce phlebitis or inflammation at the injection site upon inadvertent extravasation. Standard, commercially available electrolyte and glucose solutions are suitable for intravenous administration; biologic or colloidal fluids (e.g., blood products, protein solutions, etc.) are not recommended.
Once diluted for administration, each dose should be used within 24 hours.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
CONTRAINDICATIONS
Acyclovir Sodium Injection is contraindicated for patients who develop hypersensitivity to acyclovir or valacyclovir.
ADVERSE REACTIONS
Adult and Pediatric Clinical Trials
The adverse reactions listed below have been observed in controlled and uncontrolled clinical trials in approximately 700 patients who received acyclovir at ~5 mg/kg (250 mg/m 2 ) 3 times daily, and approximately 300 patients who received ~10 mg/kg (500 mg/m 2 ) 3 times daily.
The most frequent adverse reactions reported during administration of acyclovir were inflammation or phlebitis at the injection site in approximately 9% of the patients, and transient elevations of serum creatinine or BUN in 5% to 10% (the higher incidence occurred usually following rapid [less than 10 minutes] intravenous infusion). Nausea and/or vomiting occurred in approximately 7% of the patients (the majority occurring in non-hospitalized patients who received 10 mg/kg). Itching, rash, or hives occurred in approximately 2% of patients. Elevation of transaminases occurred in 1% to 2% of patients.
The following hematologic abnormalities occurred at a frequency of less than 1%: anemia, neutropenia, thrombocytopenia, thrombocytosis, leukocytosis, and neutrophilia. In addition, anorexia and hematuria were observed.
Neonatal Clinical Trial
In Study 2, 72 of the 88 enrolled neonates received 60 mg/kg/day. Among subjects with recorded normal baseline values, the following laboratory abnormalities were reported: 6% (4/64) with Grade 3 or 4 increase in creatinine; 4% (2/52) with total bilirubin Grade 3 or 4 toxicity; 13% (8/64) with hemoglobin < 8 gram%; 16% (10/64) and 3% (2/64) with absolute neutrophil count 500 to 1,000 cells/mm 3 and < 500 cells/mm 3 , respectively; 10% (6/63) and 5% (3/63) with platelet count 50,000 to 100,000 and < 50,000, respectively.
Observed During Clinical Practice
In addition to adverse events reported from clinical trials, the following events have been identified during post-approval use of Acyclovir Sodium Injection in clinical practice. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These events have been chosen for inclusion due to either their seriousness, frequency of reporting, potential causal connection to acyclovir, or a combination of these factors.
General: Anaphylaxis, angioedema, fatigue, fever, headache, pain, peripheral edema.
Digestive: Abdominal pain, diarrhea, gastrointestinal distress, nausea.
Cardiovascular: Hypotension.
Hematologic and Lymphatic: Disseminated intravascular coagulation, hemolysis, leukocytoclastic vasculitis, leukopenia, lymphadenopathy.
Hepatobiliary Tract and Pancreas: Elevated liver function tests, hepatitis, hyperbilirubinemia, jaundice.
Musculoskeletal: Myalgia.
Nervous: Aggressive behavior, agitation, ataxia, coma, confusion, delirium, dizziness, dysarthria, encephalopathy, hallucinations, obtundation, paresthesia, psychosis, seizure, somnolence, tremor. These symptoms may be marked, particularly in older adults (see PRECAUTIONS ).
Skin: Alopecia, erythema multiforme, photosensitive rash, pruritus, rash, Stevens-Johnson syndrome, toxic epidermal necrolysis, urticaria. Severe local inflammatory reactions, including tissue necrosis, have occurred following infusion of acyclovir into extravascular tissues.
Special Senses: Visual abnormalities.
Urogenital: Renal failure, elevated blood urea nitrogen, elevated creatinine (see WARNINGS ).
Drug Interactions
Coadministration of probenecid with acyclovir has been shown to increase the mean acyclovir half-life and the area under the concentration-time curve. Urinary excretion and renal clearance were correspondingly reduced.
DESCRIPTION
Acyclovir Sodium Injection is a synthetic nucleoside analogue, active against herpes viruses. It is a sterile, aqueous solution for intravenous infusion, containing 50 mg acyclovir per mL in Water for Injection, USP. The concentration is equivalent to 54.9 mg of acyclovir sodium per mL in Water for Injection, USP. The sodium content is approximately 5.1 mg/mL. The pH range of the solution is 10.85 to 11.50. Acyclovir Sodium Injection contains Sodium Hydroxide, NF as inactive ingredient. Further dilution of Acyclovir Sodium Injection in an appropriate intravenous solution must be performed before infusion (see DOSAGE AND ADMINISTRATION, Administration ).
The chemical name of acyclovir sodium is 9-[(2-Hydroxyethoxy)methyl] guanine, and has the following structural formula:
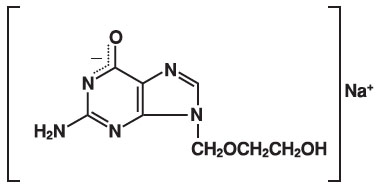
Acyclovir, USP is a white to off-white, crystalline powder. Acyclovir sodium is the sodium salt of acyclovir, which is formed in situ , with the molecular formula C 8 H 10 N 5 NaO 3 and a molecular weight of 247.19. The maximum solubility in water at 25°C exceeds 100 mg/mL. At physiologic pH, acyclovir sodium exists as the unionized form with a molecular weight of 225 and a maximum solubility in water at 37°C of 2.5 mg/mL. The pka's of acyclovir are 2.27 and 9.25.
CLINICAL PHARMACOLOGY
Pharmacokinetics
The pharmacokinetics of acyclovir after intravenous administration have been evaluated in adult patients with normal renal function during Phase 1/2 studies after single doses ranging from 0.5 mg/kg to 15 mg/kg and after multiple doses ranging from 2.5 to 15 mg/kg every 8 hours. Proportionality between dose and plasma levels is seen after single doses or at steady state after multiple dosing. Average steady-state peak and trough concentrations from 1-hour infusions administered every 8 hours are given in Table 1.
| Dosage Regimen | C SS max | C SS trough |
| 5 mg/kg q 8 h (n=8) | 9.8 mcg/mL range: 5.5 to 13.8 | 0.7 mcg/mL range: 0.2 to 1 |
| 10 mg/kg q 8 h (n=7) | 22.9 mcg/mL range: 14.1 to 44.1 | 1.9 mcg/mL range: 0.5 to 2.9 |
Concentrations achieved in the cerebrospinal fluid are approximately 50% of plasma values. Plasma protein binding is relatively low (9% to 33%) and drug interactions involving binding site displacement are not anticipated.
Renal excretion of unchanged drug is the major route of acyclovir elimination accounting for 62% to 91% of the dose. The only major urinary metabolite detected is 9-carboxymethoxymethylguanine accounting for up to 14.1% of the dose in patients with normal renal function.
The half-life and total body clearance of acyclovir are dependent on renal function as shown in Table 2.
| Total Body Clearance | |||
| Creatinine Clearance (mL/min/1.73 m 2 ) | Half-Life (h) | (mL/min/1.73 m 2 ) | (mL/min/kg) |
| > 80 | 2.5 | 327 | 5.1 |
| 50 to 80 | 3 | 248 | 3.9 |
| 15 to 50 | 3.5 | 190 | 3.4 |
| 0 (Anuric) | 19.5 | 29 | 0.5 |
Special Populations
Adults with Impaired Renal Function
Acyclovir was administered at a dose of 2.5 mg/kg to 6 adult patients with severe renal failure. The peak and trough plasma levels during the 47 hours preceding hemodialysis were 8.5 mcg/mL and 0.7 mcg/mL, respectively.
Consult DOSAGE AND ADMINISTRATION section for recommended adjustments in dosing based upon creatinine clearance.
Pediatrics
Acyclovir pharmacokinetics were determined in 16 pediatric patients with normal renal function ranging in age from 3 months to 16 years at doses of approximately 10 mg/kg and 20 mg/kg every 8 hours (Table 3). Concentrations achieved at these regimens are similar to those in adults receiving 5 mg/kg and 10 mg/kg every 8 hours, respectively (Table 1). Acyclovir pharmacokinetics were determined in 12 patients ranging in age from birth to 3 months at doses of 5 mg/kg, 10 mg/kg, and 15 mg/kg every 8 hours (Table 3).
| Parameter | Aged from Birth to 3 Months (n=12) | Aged 3 Months to 12 Years (n=16) |
| CL (mL/min/kg) | 4.46 ± 1.61 | 8.44 ± 2.92 |
| VDSS (L/kg) | 1.08 ± 0.35 | 1.01 ± 0.28 |
| Elimination half-life (hours) | 3.80 ± 1.19 | 2.36 ± 0.97 |
Acyclovir pharmacokinetic samples were collected in full-term and pre-term neonates with normal renal function who received varying dosing regimens of acyclovir for the treatment of suspected neonatal HSV infection. Model-predicted pharmacokinetic parameters stratified by post-menstrual age (PMA) are summarized in Table 4.
| Post-Menstrual Age (PMA) | n | IV Dose Administered over 1 hour. | Parameter (Median [Range]) | |||
| Cmin ss (mg/L) | Cmax ss (mg/L) | CL (L/h/kg) | V (L/kg) | |||
| < 30 Weeks | 13 | 500 mg/m 2 every 8 h or | 3.92 (2.38 to 39.3) | 10.3 (4.59 to 110) | 0.21 (0.10 to 0.31) | 2.88 (0.65 to 5.30) |
| 10 mg/kg or 20 mg/kg every 12 h | ||||||
| 30 to < 36 Weeks | 9 | 500 mg/m 2 every 8 h or | 5.10 (2.54 to 9.62) | 8.83 (5.44 to 29.8) | 0.45 (0.30 to 0.81) | 4.49 (1.87 to 10.85) |
| 10 mg/kg or 20 mg/kg every 12 h | ||||||
| or | ||||||
| 20 mg/kg every 8 h | ||||||
| 36 to 41 Weeks | 6 | 500 mg/m 2 every 8 h | 2.90 (2.19 to 7.46) | 12.4 (10.8 to 86.1) | 0.59 (0.13 to 0.77) | 2.55 (0.29 to 4.09) |
| Overall | 28 | – | 4.15 | 11.1 | 0.28 | 3.34 |
| (2.19 to 39.3) | (4.59 to 110) | (0.10 to 0.81) | (0.29 to 10.9) | |||
Geriatrics
Acyclovir plasma concentrations are higher in geriatric patients compared with younger adults, in part due to age-related changes in renal function. Dosage reduction may be required in geriatric patients with underlying renal impairment (see PRECAUTIONS:Geriatric Use ).
Drug Interactions
Coadministration of probenecid with acyclovir has been shown to increase the mean acyclovir half-life and the area under the concentration-time curve. Urinary excretion and renal clearance were correspondingly reduced.
HOW SUPPLIED
Acyclovir Sodium Injection is available as:
| NDC | Acyclovir Sodium Injection , 50 mg / mL | Packaging |
| 68382-048-10 | 10 mL | 10 vials packed in a carton |
| 68382-049-10 | 20 mL | 10 vials packed in a carton |
Storage
Store at 20°C to 25°C (68°F to 77°F) [see USP Controlled Room Temperature].
Discard unused portion.
This container closure is not made with natural rubber latex.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
Manufactured by:
Cadila Healthcare Ltd.
Ahmedabad, India
Distributed by:
Zydus Pharmaceuticals (USA) Inc.
Pennington, NJ 08534
Rev.: 06/21